 Home
Home
|
Table of Content - Volume 15 Issue 2 - August 2020
A study of outcome of thermal radiofrequency nerve ablation of genicular nerves for the management of chronic osteoarthritis of knee joint
Tsering Yougyal1*, Jasa Ram Thakur2, Vijay Kumar Sauhta3, Girish Sharma4, Shweta Mahajan5
1,2Department of Health & Family Welfare Himachal Pradesh Government, Operation Theatre Incharge Civil Hospital Joginder Nagar, Distt Mandi, Himachal Pradesh, INDIA. 3Operation Theatre Incharge Civil Hospital Theog Shimla Himachal Pradesh, INDIA. 4Professor, Department of Anaesthesia, Dr Y. S. Parmar Government Medical College, Nahan, District Sirmour, Himachal Pradesh, INDIA. 5Associate Professor, Department of Anaesthesia, Indra Gandhi Medical college, Shimla. Himachal Pradesh, INDIA. Email: yougyal1001@gmail.com. , jassathakur821@gmail.com , d.sauhta@gmail.com
Abstract Background: Genicular nerve block with radiofrequency (RF) has recently emerged as a novel alternative treatment for chronic knee pain. Present study evaluates analgesic intake in thermal Radinfrequency ablation of genicular nerve in osteoarthritis of knee joint. Aim and objective: To compare the total analgesic intake in Thermal Radiofrequency ablation of genicular nerve with control group in patients with osteoarthritis of knee joint. Methodology: Present study was a controlled prospective randomized double blinded study carried out 0n patients diagnosed clinically with osteoarthritis of knee. In Group I, No thermal or Pulsed radiofrequency was given. In Group II, Radiofrequency was given with target temperature at 70 degree Celsius for three cycles each of 1.5 minutes duration. Data was analysed with appropriate statistical tests. Results and discussion: The patients of group I started complaining of pain at one week of follow up and were not satisfied and had to use similar amount of rescue analgesic capsules for pain control that they were using prior to procedure. They complained of progressive rise in pain in the affected knee joint during the consecutive follow up at 4th, 8th and 12th week. Key Word: thermal radiofrequency nerve ablation.
INTRODUCTION More than 50% of the world population above age of 65 years show X-ray evidence of OA in one of the knee joints, thus demonstrating the high incidence of this disease. While OA knee joints is equally present in men and women, it appears to be more common among younger men (<45years) and in the older women (>45 years). 1 Over 40% of the Indian population in the age group of 70 years or above suffer from OA. Nearly 2% of these develop severe knee pain and disability. As per a statement quoted by Piramal Healthcare Limited in a nationwide campaign against chronic diseases, “India is expected to be the chronic disease capital, with 60 million people with arthritis, by 2025. Persons aged >65 years are more commonly affected by knee OA, as there is overall increase in life expectancy; there is an alarming trend for future growth in the prevalence of knee OA in older population to be seen. 2 Currently 80% of persons affected by OA knee joint already report having some movement limitation, and 20% report not being able to perform major activities of daily living.3 OA can be seen as a degenerative, chronic, and often progressive joint disease. The guidelines for treatment of OA outlined the use of nonpharmacologic modalities, as well as the use of pharmacologic agents. The primary objective in clinically managing patients with OA of the knee involves controlling pain and swelling, improving quality of life, improving physical capacity, and preventing progression of the arthritis. For many patients with OA, the relief of mild-to-moderate knee joint pain afforded by the simple analgesic, acetaminophen, is comparable with that achievable with an NSAID. 4-8 Other Medications used are intraarticular glucocorticoids and chondroitin and glucosamine (orally). 9-12 As a general concept, pain treatment by radiofrequency (RF) energy has had wide coverage in the pain management practice for the past 30 years. 13 Genicular nerve block with radiofrequency (RF) has recently emerged as a novel alternative treatment for chronic knee pain. Not much of studies of such nature have been performed to determine the effectiveness of the thermal radiofrequency nerve ablation of genicular nerves for the management of chronic osteoarthritic of knee joint. Aim and objective: To compare the total analgesic intake in Thermal Radiofrequency ablation of genicular nerve with control group in patients with osteoarthritis of knee joint
MATERIAL AND METHODS Present study was a controlled prospective randomized double blinded study carried out 0n patients diagnosed clinically with osteoarthritis of knee. The study was carried out in the pain clinic centre of Indra Gandhi medical college and hospital Shimla from the period July 2016 to Jan 2017. Inclusion criteria: 1. Patients between Stage 1 and Stage 3 radiological changes, according to the Kellgren-Lawrence classification 13 2. Patients with Age from 40 to 70 years.3. Patients with Pain localised to knee joint with no referred pain. 4. Patients without visible gross structural deformity of the knee joint. 5. Patients within ASA Grade I and II. 6. Patients on conservative treatment such as physical therapy, analgesic drugs including NSAIDs or opioids, for at least six months Exclusion criteria: 1. Patients refusal for the intervention. 2. Patients at Stage 4 radiologically, according to the Kellgren Lawrence classification. 3. Patients with Age less than 40 and more than 70 years. 4. Patients with visible gross deformity of the knee joint. 5. Patients of ASA Grade III or more. 6. Existence of general contraindications against application of invasive intervention 7. Psychiatric disorders. Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining study to them. Under all aseptic condition, knee joint palpated, needle insertion sites were marked with C-Arm guidance, nerve targeted included superior lateral genicular nerve, superior medial genicular nerve and the inferior medial genicular nerve. A radiofrequency cannula with 22 G 100-mm length and 10-mm active tip (Cosman RFK, Cosman medical inc, USA) was used for the procedure. In Group I, after localising the Genicular nerve, 1 ml of 1% lidocaine was given at each of the three needle sites and waited for two minutes. No thermal or Pulsed radiofrequency was given and patient shifted to the recovery room. In Group II, after localising the Genicular nerve, 1 ml of 1% lidocaine was given at each needle site and waited for two minutes. Radiofrequency was given with target temperature at 70 degree Celsius for three cycles each of 1.5 minutes duration.
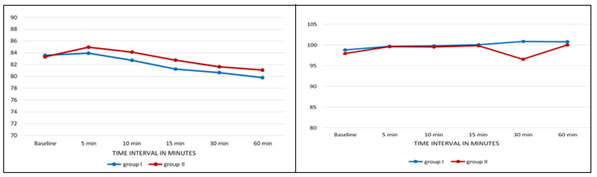
RESULTS In this study, both the groups were comparable in demographic variables like age, weight and sex. There were more number of female patients in both the group with total number of 31 out of total 50 patients (i.e. 62%) and 19 out of 50 patients (i.e. 38%) were males. Both the group were comparable and statistically insignificant (p values >0.05). General physical examination and investigation of all the patients were within normal limits. Out of the 50 patients recruited for the study, 15 patients (30 %) were ASA I and 35 patients (70%) were ASA II. The baseline heart rate (Table V) was 83.56 ± 5.760 bpm and 83.32 ± 5.956 bpm in group I and group II respectively with p value = 0.885. The baseline mean arterial pressure was 98.76± 8.084 mmHg and 97.92 ± 9.151 mmHg in group I and group II respectively with p value = 0.732. The baseline mean Spo2 was 94.44 ± 2.162 % and 94.72 ± 2.264 mmHg in group I and group II respectively with p value = 0.657. All these baseline parameters were comparable in both the groups. The mean heart rate during the procedure (Table VI) at 0, 5, 10, 15, 30 and 60 minutes in group I was 83.56 ± 5.760, 83.92 ± 5.492, 82.72 ± 6.127, 81.24 ± 5.703, 80.64 ± 5.155 and 79.80 ± 5.050 bpm respectively and in group II was 83.32 ± 5.956, 84.96 ± 5.955, 84.12 ± 6.540, 82.76 ± 6.064, 81.64 ± 5.514 and 81.08 ± 4.636 bpm respectively. The mean heart rate initially and during the procedure was statistically insignificant and comparable amongst the two groups. (fig 1) The mean arterial pressure (MAP) during the procedure (table VII) at 0, 5, 10, 15, 30 and 60 minutes in group I was 98.76 ± 8.084, 99.64 ± 8.779, 99.76 ± 9.858, 100.00 ± 9.631, 100.80 ± 9.552 and 100.72 ± 8.581 mmHg respectively and in group II was 97.92 ± 9.151, 99.56 ± 9.152, 99.48 ± 10.504, 99.80 ± 10.673, 96.52 ± 21.176 and 99.96 ± 8.900 mmHg respectively. The mean arterial pressure initially and during the procedure was statistically insignificant and comparable amongst the two groups. (fig 2) The mean respiratory rate of the patients during the procedure (table VIII) at 0, 5, 10, 15, 30 and 60 minutes in group I was 16.44 ± 1.158, 16.92 ± 1.187, 16.72 ± 1.100, 16.40 ± 1.080, 16.44 ± 0 .917 and 15.76 ± 1.200 per minute respectively and in group II was 16.88 ± 1.236, 17.28 ± 1.173, 16.72 ± 1.208, 16.60 ± 1.258, 16.80 ± 1.118 and 16.24 ±.723 per minute respectively. The mean respiratory rate initially and during the procedure was statistically insignificant and comparable amongst the two groups. (table 1) The mean oxygen saturation (Spo2) initially and during the procedure (Table IX) at 0, 5, 10, 15, 30 and 60 minutes in group I was 94.44 ± 2.162, 95.96 ± 2.010, 96.40 ± 2.102, 96.68 ± 1.773, 96.68 ± 1.887, 96.60 ± 1.936 percentage respectively and in group II was 94.72 ± 2.264, 96.12 ± 1.878, 96.44 ± 2.063, 96.68 ± 1.773, 96.68 ± 1.887 and 96.80 ± 1.803 percentage respectively. The mean oxygen saturation (Spo2) initially and during the procedure was statistically insignificant and comparable amongst the two groups. (table 2) The mean consumption of capsule Raceclo as rescue analgesic in Group I and Group II initially was 6.44±0.917 and 6.44± 0.961 respectively, showing no significant intergroup difference statistically (p- value=1.000). In the group I, the mean consumption of capsule raceclo at one week follow up was 5.52 ± 0.823 with the baseline initial consumption of 6.44 ± 0.917 and was statistically significant (p = 0.001) while in group II the mean consumption at one week was 0.60 ± 1.190 from the baseline consumption of 6.44 ± 0.961, was statistically significant (p value = 0.001). When both the groups were compared for the mean consumption of capsule raceclo at one week follow up period, the change was statistically significant with p value of 0.001. In the group I, the mean consumption of capsule raceclo at 4th, 8th and 12th week follow up were 6.16 ± 0.746, 6.28 ± 0.737 and 6.68 ± 0.690 respectively, which were almost similar to the baseline initial consumption of 6.44 ± 0.917 and were statistically insignificant (p >0.05). In group II, the mean consumption of capsule raceclo at 4th, 8th and 12th week follow up were 0.56 ± 1.356, 0.96 ± 1.567 and 1.52 ± 1.447 respectively, with the baseline initial consumption of 6.44 ± 0.961 (p value < 0.05), which were statistically highly significant. When both the groups were compared for the mean consumption of capsule raceclo at 4th, 8th and 12th week follow up period, the change was statistically significant ( p value of 0.001). (table 3) In this study all the patient used Tablet Raceclo as rescue analgesic and didn’t require Tablet Contramal. (table 4) Figure 1: Comparison of heart rate between two groups Figure 2: Comparison of Mean Arterial Pressure (MAP) in two groups
Table 1: Comparison of Respiratory Rate (RR) in two groups
Table 2: Comparison of Oxygen Saturation (SPO2) in two groups
Table 3: Comparison of Capsule Raceclo consumption in a week in two groups
Table 4: Comparison of Tablet Contramal consumption in a week in two groups
DISCUSSION We compared the requirement of rescue analgesic in the form of Capsule Racelclo containing Aceclofenac sodium 100 mg of sustained release pellets and Rabeprazole 20 mg enteric coated pellets, prescribed to be used once a day after meal. The mean consumption of rescue analgesic prior to procedure was 6.44 ± 0.917 in group I and 6.44 ± 0.961 in group II, which was comparable (p value = 1.000). The mean consumption at 1st week follow up was 5.52 ± 0.823917 in group I and 0.60 ± 1.190 in group II and was statistically significant (p value = 0.000). In the 4th week follow up, the mean consumption of rescue analgesics was 6.16 ± 0.746 in group I and 0.56 ± 1.356 in the group II and was statistically highly significant (p value = 0.000). In the 8th week follow up, the mean consumption of rescue analgesics was 6.28 ± 0.737 in group I and 0.96 ± 1.567 in the group II and was statistically highly significant (p value = 0.000). In the 12th week follow up, the mean consumption of rescue analgesics was 6.68 ± 0.690 in group I and 1.52 ± 1.447 in the group II and was statistically highly significant (p value = 0.000). The requirement of rescue analgesia in both groups were comparable till post procedure period of 2 to 3 days ( in less than a week duration post intervention ), after that there was significant difference with the use of rescue analgesic on consecutive follow up with the p value at follow up at 1st week, 4th week, 8th week and 12th week as 0.000 consistently which is statistically highly significant, implying that there is significant decrease in the usage of rescue analgesic in the group II patients after the radiofrequency ablation of genicular nerves of the affected knee joint. There was provision of a back up analgesia as tablet tramadol 50 mg SOS (tablet Contramal by Abbot) which could be given to maximum limit of 400 mg/day. In our study, all the patients of group I and group II never had to use tablet Tramadol during the course of study. The RF thermal ablation procedure of genicular nerves of knee joints is an effective, safe, and minimally invasive method that can be applied to the patients with osteoarthritis-related chronic knee pain when there has been insufficient response to conservative treatment and is presently a promising intervention for patients with chronic painful knee osteoarthritis. All the previous similar studies worldwide in different countries, most famously by Choi et al., Wen-Sheng Shen et al., Pakize KIRDEMİR et al. and Ferdinand Iannaccone et al., concluded with the same results and recommendations.14-17
CONCLUSION Radiofrequency thermal ablation of genicular nerves of knee joint provides excellent analgesia in patients with osteoarthritis- related chronic knee pain.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.