 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 3 Issue 2 -September 2017
Role of Inj. Dexamethasone for prevention of post operative nausea and vomiting in laparoscopic surgeries
Manohar Mane1*, Divakar Patil2, J Paranjape3, Ravikiran Thote4
1Associate Professor, 2Professor, 3Professor and HOD, 4Sr. Resident, Department of Anesthesiology, Bharati Vidyapeeth Deemed University Medical College and Hospital Sangli, Maharashtra, INDIA. Email: manoharmane2002@yahoo.co.in
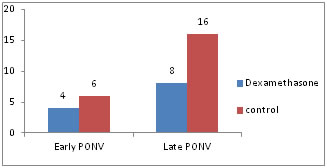
Abstract Aims and Objectives: To study the role of inj. Dexamethasone for early and late Post Operative Nausea and Vomiting in laparoscopic surgeries. And also to record side effects of dexamethasone. Study Design: Prospective, randomized, double blind trail. Material And Methods: Total 80 patients of ASA physical states I and II were randomly allocated to two groups of 40 each. After induction of general anesthesia, Group D received 8 mg/kg Dexamethasone, Group C received normal saline 2 ml. Both the groups were compared on the basis of vomiting up to 6 hrs after conclusion of surgery (Early PONV), and 6 hrs to 24 hrs after surgery (late PONV).Also the side effects i.e. infection at port site, or any bleeding from wound was recorded. Results: Post operative nausea and vomiting up to 6 hrs in Group D was 4 as compared to 6 in Group C. While incidence of late PONV was 8 in Group D Vs 16 in Group C which is statistically significant. No patient in any group had wound infection or bleeding from port site in postoperative period. Conclusion: Inj. Dexamethasone effectively reduces late post operative nausea vomiting, without any added evidence of side effects. Key Words: Dexamethasone, postoperative nausea vomiting (PONV), laparoscopy.
INTRODUCTION Laparoscopic surgeries have many advantages like it is less invasive,, less handling of the intra abdominal organs, decreased post operative pain and lesser chances of postoperative adhesions. But the incidence of postoperative nausea and vomiting are also increased in a patient who have undergone laparoscopic surgeries(1,2,3).Causes that may contribute to post operative nausea and vomiting (PONV) are Anesthesia related causes like the use of opioid drugs, nitrous oxide. Patient related causes - Female gender, h/o motion sickness, h/o PONV, non smokers3,4. Incidence of PONV is reported to be 30-40 %, while in high risk patients it is as high as 70 %.1,5 PONV is one of the distressing complaints in post operative period. It may lead to aspiration, increased morbidity, wound dehiscence and gaping, increased hospital stay or readmission. Many drugs are in use to prevent PONV like 5HT3 antagonists, antihistaminic, antiemetic and dexamethasone etc.6,7,8,9. Dexamethasone, is a steroid drug also having beneficial effect for prevention of PONV10,11. Though the exact mechanism of action is not known, the proposed hypothesis are central or peripheral inhibition of the production or secretion of serotonin by releasing endorphins and central inhibition of synthesis of prostaglandins or changes in the permeability of the blood brain barrier to these serum proteins. Its anti-emetic action, at least in part, may be elicited via the blockage of corticosteroid receptors in the nucleus tactus-solitarius of the CNS5. Dexamethasone may also exert its anti-emetic action through some peripheral mechanisms. It has strong anti-inflammatory effects and may significantly reduce inflammation around the surgical sites and does reduce the ascending parasympathetic impulses (Vagus) to the vomiting center and PONV. Dexamethasone is found to be more effective when administered before induction Also it has been shown to decrease the requirement of analgesic drugs in post operative period. The inherent risks of dexamethasone include infection and adrenal suppression. However no report of complications associated with a single bolus of dexamethasone is reported so far. Recent studies have shown that combination of dexamethasone with Ondansetron is more effective for prevention of PONV than monotherapy.4,12,13 Inclusion Criteria
Exclusion Criteria
MATERIALS AND METHODS Total 40 patients were studied. Informed written consent was taken. In operation theatre, IV line was secured, standard monitors were applied. All the patients were premeditated with inj. Glycopyrrolate 0.2 mg inj. Midazolam 0.03 mg/kg, inj. Pentazocine 0.3 mg/kg, inj. Ranitidine 50 mg,- inj. Ondansetron 4mg iv,. Patients were divided in to two groups randomly, group D received inj. Dexamethasone 2 cc (8 mg iv). Group C received normal saline 2 cc. All patients were oxygenated with 100 % oxygen for 5 minutes, and then induced with inj. Propofol 2mg/kg., and paralyzed with inj. Succinylcholine 1 mg/kg. Intra operatively anesthesia was maintained with oxygen and nitrous oxide (60: 40), sevoflurane. Vecuronium was used as muscle relaxant. Inj diclofenac 75 mg given IM at the time of end of the surgery and then 12 hourly. At the end of surgery patients were reversed with inj. Neostigmine 0.05 mg/kg plus inj. Glycopyrrolate 8 microgm/kg. and then patients extubated and shifted to PACU. Incidence of PONV is recorded up to first 6 hours as early PONV and then 6 hrs to 24 hrs as late PONV. Nausea defined as the subjectively un-pleasant sensation associated with awareness of the urge to vomit whereas vomiting was defined as the forceful expulsion of gastric contents from the mouth. Retching i.e. diaphragmatic twitching without expulsion of gastric contents will be noted as vomiting. Side effect in the form of infection at port insertion site is noted at the time of stitch removal. Table 1: Demographic data
Types of Operation – Lap.cholecystectomy, Lap. Appendicectomy, Lap. hystrectomy,adhesiolysis Dignostic lap. Lap. Hernia, ovarian cystectomy
Table 2: Duration of Surgery – (average)
Duration of surgery is comparable in both groups.
Table 3: Incidence of Nausea and vomiting (Up to 6 Hrs)
p>0.05 Table 4: Incidence of Nausea and Vomiting (6-24 Hrs)
P< 0.05
Table 6: Incidence of infection
DISCUSSION Postoperative nausea and vomiting is one of the distressing symptom. Incidence of PONV is up to 20 – 70 %. It may add to the hospital stay and increases economic burden on patient. By decreasing postoperative nausea vomiting we can make the patient comfortable. Many drugs have been used to decrease PONV namely Ondansetron, metoclopramide, haloperidol, dexamethasone. In the current study, we compared dexamethasone with or without Ondansetron, from this study it can be seen that addition of dexamethasone is helpful especially to decrease the incidence of late PONV. Our results are comparable with study done by B Gautam et al12, which also concluded that combination of dexamethasone to ondansetron is more effective for prevention of PONV in laparoscopic cholecystectomy patient. Mohammad eidy et al14 in their study also found that addition of dexamethasone to ondansetron gives better protection against PONV. Gupta P et al15, and Wanderlay Marques Bernardo et al2 also concluded in their study that preoperative dexamethasone decreases PONV. DeOliveira GS Jr et al16 studied different doses of dexamethasone and found that 4-5 mg dose has same results compared to that of 8-10 mg for prevention of PONV. Dexamethasone has been studied in combination with other antiemetics also, like metoclopramide and haloperidol and found to decrease the incidence of PONV17. In contrast to our study results, Souvic Maitra et al10 in ther metaanalysis found that dexamethasone is only effective for prevention of nausea while the incidence of vomting and rescue antiemetics requirements are same for both groups. Cristoph Czarnetzki et al18 studied role of dexamethasone for PONV in post tonsillectomy patients, concluded that it decreases the risk of PONV but they also reported that incidence of post tonsillectomy bleeding is also increased.
CONCLUSION Dexamethasone effectively decreases the incidence of late PONV when given preoperatively, without any side effects.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.