 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 8 Issue 3 - December 2018
Effect of intra-articular fentanyl in combination with dexmedetomidine on postoperative analgesia after arthroscopy knee surgery
Anupama Sahasrabudhe1*, Shwetha K M2, Smith Kadakia3
1Associate professor, 2Assistant Professor, 3PG student, Department of Anaesthesiology, D. Y. Patil Medical College, Kolhapur, Maharashtra. Email: dranuds@gmail.com
Abstract Background: Dexmedetomedine has been used as sole agent as well as adjuvant to another drug in several studies to enhance postoperative analgesia after knee arthroscopy with an increasedtime for the requirement of first rescue medication and a decreased need for postoperative analgesia4,5. Fentanyl is a potent and cheap available opioid which can provide regional analgesia by acting on peripheral opioid receptors. Objectives: To investigate effect of intra-articular Fentanyl in Combination with Dexmedetomidine on postoperative analgesia after arthroscopy knee surgeryResults: Combination therapy reduces need for rescue medication in first 6 hours postoperative with no patients needing rescue medication in first 4 hours. The mean VAS score in study group was found to be 3.815. Conclusions: Combination therapy is hypothesized to have better and longer postoperative analgesic effects Key Word: Dexmedetomedine, Fentanyl, Visual Analogue Scale
INTRODUCTION Intra-articular administration of local anaesthetic is a unique method of providing better analgesia post knee arthroscopy to reduce consumption and side effects of analgesics. Various analgesic drugs have been used in this regard including local anesthetics, opioids, NSAIDS etc.1More recently, long duration analgesia has been achieved using intra articular morphine, although the result with plain morphine have not been significant. The use of intra articular morphine and bupivacaine in combination has shown significant result post knee arthroscopy. Contrary to this, other investigators have failed to demonstrate an analgesic effect of intra articular morphine.2 Another advent in post-arthroscopy analgesia includes multimodal pain analgesia. The importance regarding this therapy is to provide sufficient analgesia by additive or mainly synergistic effects of different analgesics, concomitantly reducing the side effects of each drug because of reduced dosage of each drug. Common combinations of local anesthetics with drugs like Fentanyl, Morphine, Ketorolac etc. have been tried with good results.3 Dexmedetomidine is a potent and highly selective alpha 2 adrenoreceptors agonist. It has sedative- hypnotic, anxiolytic and analgesic, anaesthetic-reducing and sympatholytic effects. Intra-articular Dexmedetomedine has been used as sole agent as well as adjuvant to another drug in several studies to enhance postoperative analgesia after knee arthroscopy with an increased time for the requirement of first rescue medication and a decreased need for postoperative analgesia4,5. Fentanyl is a potent and cheap available opioid which can provide regional analgesia by acting on peripheral opioid receptors. The systemic side effects of Fentanyl can be avoided by giving it Intra-articular6.The primary aim of our present study is to investigate the efficacy of a Dexmedetomedine when used with Fentanyl intra-articularly on post-operative pain intensity after knee arthroscopy. MATERIAL AND METHODS This studywas undertaken on 30 consenting adult inpatients of Dr. D.Y. Patil Hospital and Research Institute posted for elective knee arthroscopy, under spinal anaesthesia from May 2015 to May 2017.Following approval of institutional ethical committee, 30 adult patients fulfilling the inclusion criteria were selected for the study. Informed consent was taken. All necessary investigative work up was done. Patients were introduced to the VAS scale prior to the surgery, the scale is a continuous scale comprised of a horizontal (HVAS) or vertical (VVAS) line, usually 10 centimetres (100 mm) in length. The scale is most commonly anchored by “no pain” (score of 0) and “pain as bad as it could be” or “worst imaginable pain” (score of 10). The VAS score was noted both at rest and at movement. Arthroscopic procedures will be carried out under spinal anesthesia using bupivacaine 0.5% heavy 3 ml. Intra operative sedation will include Inj. Midazolam 2 mg administered intravenously. Intra articular analgesic solution (Fentanyl 100mcg+50microgram Dexmedetomidine diluted to 10ml.) will be instilled at the end of surgery during suturing phase. Tourniquet will be kept inflated for 15 min for fixation of drug to synovial membrane. Visual Analogue Scores were recorded preoperatively (baseline) and at 1hr, 2hr, 3hr, 4hr, 5hr, 6hr, 7hr, 8hr upto 14hrs after the intra articular injection. Patients were given rescue medication when VAS score was more than 4. The Initial rescue medication was 75mg Diclofenac Intramuscularly. In the event of insufficient analgesia 100 mg Tramadol intravenously given over 10 minutes. The time for the first request for analgesia and total analgesic requirement will be recorded at the same time the VAS would be noted marking the end of the study for that particular patient. Statistical methods Convenient sampling was done. Total 30 patient were randomly selected for this study. Descriptive statistical analysis has been carried out in. All the statistical analysis of data was done with programming software SPSS version 15.0 and graphical representation was done using Microsoft excel 7.0. Associations were done using student ‘t’ test. RESULTS Table 1: Distribution of age and sex among the study population
No any significance was seen in socio demographic variables.
Table 2: Description of pain score for all the patients across 6 hours
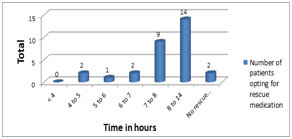
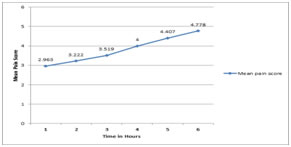
Refers to the number of patients present in the study at each particular time interval. When patients requested for rescue medications, VAS score was recorded and no further VAS scores were measured in that particular patient. At the first, second, third and fourth hours thirty patients were present in the study, 27 patients were left at the end of 6 hours. Figure 1: Time and frequency of patients who opted for rescue medication No patient in first 3 hours opted rescue medications. At 4-5 hours 2 patients opted for rescue medications. At 5-6 hours 1 patient opted for rescue medications. At 6-7 hours 2 patients opted for rescue medications. After seven hours 5 patients opted for rescue medications. Figure 2: Means Plot of Pain Score during the first 6 post-operative hours and after 6 post-operative hours. The mean VAS score in study group was found to be 3.815. Mean VAS scores of the patients was below 4 in the first four hours rising above 4 subsequently.
DISCUSSION In the present study 30 patients received combination therapy of Fentanyl with Dexmedetomidine administered intra-articularly. In the present study demographic data showed no significance. In our study only 3 patients (10%) opted for rescue medications within six hours of surgery and 27 (90%) opted for rescue medications six hours after surgery. Al-Metwalli et al.7 in2008 performed studied using intra-articular dexmedetomidine, intravenous dexmedetomidine and placebo, and concluded that dexmedetomidine when given intra-articularly gave longer postoperative pain free state and also reduced the need for rescue medication. We also found similar results with zero patient needing rescue medication in first four hours post operatively. Thus these result support our study. Also similar results were seen in the study done by Paul et al.4 who concluded that dexmedetomidine when administered intra articularly as an adjunct to ropivacaine in patients posted for arthroscopic knee surgery improved both the efficacy of ropivacaine and duration of postoperative analgesia. Alipour etal8 in 2014 evaluated the efficacy of intra-articular dexmedetomidine and showed that synergistic effect with lesser use of rescue medication. Sun et al 9 in 2012 studied the efficacy and safety of a single dose of clonidine, concluded its analgesic effect is for duration lasting for just 4 h. It showed significant hypotension post operatively thereby reducing its usage. On the contrary, using intra-articular dexmedetomidine in our study provided more effective and prolonged analgesia without showing any systemic side effects.In the present study the mean VAS score 3.815. The Mean VAS score at Sixth hour after surgery in was 4.778 which was similar to the findings of Huey Ping et al3where the VAS scores were lower up to 8 hours postoperatively. He studied analgesic efficacy of a combination of ropivacaine, morphine, and ketorolac with plain ropivacaine or bupivacaine and concluded that addition of Intra-articular Morphine and Ketorolac to Ropivacaine improved analgesic duration of LA, reduced use of recue medication arthroscopic knee surgery. Yari Met al10 recorded VAS scores at 1, 2, 4, 6 and 24 hours after surgery, they found out that administering of 15 mg morphine intra-articularly post knee arthroscopic surgery considerably prolonged the analgesia duration and lesser use of rescue medication. Samoladas EP et al11 assessed the pain using the VAS score at intervals of 1,2,3,4 and 6 hours after the operation and recorded the need for extra analgesia. The study stated that local anaesthetic when administered intra-articularly provided better pain control post knee arthroscopy. Therefore Multimodal analgesia is favoured in regards to effective treatment of postoperative pain. The reason behind this is to attain adequate analgesia due to the synergistic property between various analgesics with subsequent reduction in dose of any individual drug required to attain the same effect as seen with Kehlet H12. Therefore a combination of Fentanyl with Dexmedetomidine administered intra-articularly was hypothesized to have better and longer postoperative analgesic effects. None of the patients in our study showed any adverse effects like nausea, vomiting, pruritus which shows safety and efficacy of this combination therapy.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.