 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 1 - January 2018
Creatinine estimation by compensated Jaffe method and enzymatic method - A comparative study
D Merriwin1, P M Abraham Sam Rajan2*, N Ananthi3
1PG Student, 2Associate Professor, 3Professor and HOD, Department of Biochemistry, Saveetha Medical College, Saveethanagar, Thandalam, Chennai – 602105, Tamil Nadu, INDIA. Email: salomi.jayasam@gmail.com
Abstract Background: Chronic Kidney Disease is a global threat to health particularly for developing countries, since therapy is expensive and life-long. Incidence of CKD has doubled in the last 15 years. Accurate creatinine measurement is essential in the diagnosis of chronic kidney disease as serum creatinine is used for estimating glomerular filtration rate. The aim of our study was to compare the analytical performance between the enzymatic method and compensated Jaffe method for estimation of creatinine. Methods: In our study we measured serum creatinine in 135 serum samples by both enzymatic and compensated Jaffe methods using Cobas c311 automated analyser. Results: Relationship between both the methods using Cobas c311 automated analyser showed a correlation coefficient of 0.999, which means these two methods correlate very well. Conclusion: There was a good agreement and comparability between compensated Jaffe and enzymatic methods except for a minimal variation at higher concentrations of creatinine. Key Words: Creatinine, Compensated Jaffe, Enzymatic method.
Chronic Kidney Disease is a worldwide problem that carries a major risk for cardiovascular morbidity and death.1,2 In India, it has been estimated that the incidence rate of end stage renal disease to be 229 per million population (pmp)3,4, and >100,000 new patients enter renal replacement programs every year in India.3,5 Current guidelines define chronic kidney disease as kidney damage or glomerular filtration rate [GFR] less than 60 ml/mint/1.73m2 for consecutive three months or more, regardless of the cause.1,2,6,7,8 Estimation of serum or plasma creatinine is most commonly used to assess renal function.1,2,6,7,8 Creatinine is a better marker of renal function than urea because its blood concentration is not significantly affected by nonrenal factors9 and shows little or no response to dietary changes. Kidney Outcomes Quality Initiative and National Institute (KDOQI) and National Institute for Health Excellence recommend to use serum creatinine concentration to estimate GFR which can be used to classify CKD into five stages (KDOQI guidelines).20 Hence accurate estimation of creatinine is very essential in a clinical laboratory. Various methods were described for estimating creatinine in biological fluids. Jaffe reaction first described in 1886, is nonspecific and has major analytical problems due to many positive and negative interferences.10 Chromogenic interferents more than 50 have been identified.11 Original Jaffe method have been modified and developed to reduce interferences, but they vary in their degree of success. In order to overcome some of the problems inherent in the Jaffe based method, compensated Jaffe and enzymatic methods have been developed for determination of creatinine.11 The objective of this study was to compare the analytical performance of the enzymatic method with compensated Jaffe method for serum creatinine estimation and whether compensated Jaffe method could be routinely used in the laboratory.
MATERIALS AND METHODS In our study serum creatinine was estimated in 135 serum samples received in the clinical biochemistry laboratory, Saveetha Medical College and Hospital by both compensated Jaffe and enzymatic method [creatininase – H2O2] using Roche Cobas c311 automated analyser. Compensated Jaffe principle: In alkaline solution, creatinine forms a yellow- orange solution with picrate[creatinine picrate].The rate of dye formation is proportional to the creatinine concentration in the specimen. Creatinine + picric acid ---–alkaline pH----→ yellow orange complex. The assay uses ‘rate blanking’ to minimize interference by bilirubin. To correct non-specific reaction including proteins and ketones, the rsults for serum or plasma are corrected by substracting 0.3mg/dl[-26µmol/L]. Principle of enzymatic method Creatinine + H2O ----Creatininase--→ Creatine Creatine + H2O ---Creatinase--→ Sarcosine + Urea Sarcosine + O2 + H2O ---Sarcosine oxidase---→Glycine + HCHO + H2O2 H2O2 + 4 - aminophenazone + HTIB ---peroxidase---→ Quinone imine chromogen + H2O + HI [HTIB – 2,4,6 triiodo -3 – hydroxybenzoic acid] The enzymatic method is based on the conversion of creatinine with the aid of creatinase, creatininase, sarcosine oxidase to glycine, formaldehyde and hydrogen peroxide. Catalyzed by peroxidase, the liberated hydrogen peroxide reacts with 4 aminophenazone and HTIB to form a quinone imine chromogen. The colour intensity of the quinone imine chromogen formed is directly proportional to the creatinine concentration in the reaction mixture.10 Quality control was done using level 1 and level 2 Biorad quality control materials. The results were analysed statistically using SPSS windows [version 17] and method validator.
RESULTS The serum creatinine levels ranged from 0.31- 11.08 mg/dl in compensated Jaffe and 0.37 – 10.8 mg/dl in enzymatic method. The mean and SD of the compensated Jaffe was 2.64 and 2.59 respectively and that of the enzymatic method was 2.66 and 2.60 respectively.
Table 1: Mean and standard deviation by compensated Jaffe and enzymatic methods
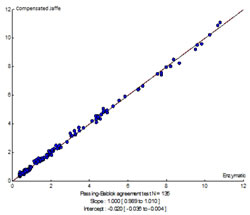
Analytical performance of the two methods namely compensated Jaffe and enzymatic methods for the estimation of creatinine were compared using Passing Bablok and Bland Altman plots. Figure 1: Passing Bablok regression analysis
Table 2: Comparison between compensated Jaffe and enzymatic methods for estimation of creatinine
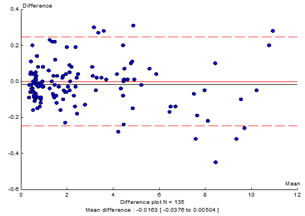
The enzymatic and compensated Jaffe methods correlate very well with a correlation coefficient of 0.999 and a slope of 1.0. Bland Altman plot: In this approach, differences are plotted against the average result obtained by two methods.
Figure 2: Bland Altman plot: Enzymatic method and compensated Jaffe method correlate very well except for a minimal variation at higher values of creatinine. DISCUSSION The method commonly used for the creatinine estimation makes use of Jaffe reaction. But Jaffe method is nonspecific and it doesn’t measure the true creatinine. It is subjected to positive interference by compounds like acetoacetate, acetone, ascorbate, glucose, protein, haemoglobin, cephalosporins and pyruvate. Bilirubin is a negative interferent with Jaffe reaction.12It can be managed by using potassium ferricyanide prior to the Jaffe reaction.12 Despite these problems the kinetic Jaffe is used since it is less expensive, rapid and easy to perform.10 Several approaches have been used to improve the specificity of Jaffe reaction like (1) absorption of creatinine into hydrated aluminium silicate[Lloyd’s reagent],(2) acid blanking, (3) oxidation of interferants with cerium sulfate.12 In compensated Jaffe method a fixed concentration is automatically substracted from each result assuming that the non creatinine chromogen interference is a constant between samples. The assay uses ‘rate blanking’ to minimize interference by bilirubin. To correct non-specific reaction, including proteins and ketones, the results for serum or plasma are corrected by substracting 0.3mg/dl[-26 µmol/L].12 Enzymatic method, a multistep approach leading to a photometric equilibrium is a more specific and accurate method to estimate serum and urine creatinine since it measures true creatinine. Enzymatic method uses smaller sample volume and hence a rapid sample throughput.12 There are comparative studies between enzymatic and kinetic Jaffe method. Although the enzymatic methods are more expensive, they are used with their lower reagent requirement and are of free of interference from substances like glucose and acetoacetate. Hence we wanted to find whether compensated Jaffe is comparable with enzymatic method so that we could use it routinely in the laboratory for the estimation of creatinine. Evaluation of the results obtained in the study proved that there is a very good correlation between both enzymatic and compensated Jaffe methods with a correlation coefficient of 0.999[R2 = 0.999].However at higher concentrations of serum creatinine, there is some variation between both the methods.
CONCLUSION From the above results and discussion it is concluded that there is good correlation between compensated Jaffe and enzymatic methods for the estimation of creatinine except for a small variation at higher concentrations of creatinine. Ethical Approval This study was carried out at clinical biochemistry laboratory of Saveetha Medical College and Hospital, Chennai over a period of six months after obtaining the approval from Institutional Ethical Committee. The article does not contain any studies with human participants or animals performed by any of the authors,
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.