 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 2 - February2018
Lipid profile patterns in university students
Gulam Saidunnisa Begum1, Chetan kumar2*, Amtul Rahaman3, Ayesha Jabeen4
1Associate Professor, 2*Tutor, 3,4Assistant Professor, Department of Biochemistry, Mahavir Institute of Medical sciences, Vikarabad, Telangana State, INDIA. Email: gulambegum1967@gmail,com
Abstract Background: Early detection of lipid imbalance should begin in adolescence in order to focus on long-term prevention of atherosclerosis by controlling the risk factors. Aim: The present study was, designed to study lipid profile and prevalence of dyslipidemia among the university students in the age group of 19-21 years. Methods: This is a cross-sectional study, which was conducted in 126 adolescents age group of 19-21 years university students in Telangana state. After getting permission from institution ethics committee, fasting blood samples were analyzed for lipid profile. Results: Mean serum cholesterol in 126 students was 156.45+ 23.43 mg/dl, mean LDL-C was 89.92+ 22.73 mg/dl, mean VLDL 16.36+ 4.82 mean triglycerides were 81.86+ 24.08 mg/dl and mean HDL-C was 50.13+5.06 mg/dl. The overall results revealed normal. Conclusions: The outcome of this study is most students attending this University, conduct a healthy lifestyle. Consuming a balanced diet, staying hydrated, and getting adequate amount of sleep, together with exercise and a healthy lifestyle will ensure both physical and mental health. Key Words: Lipid profile, university students, National Cholesterol Education Program (NCEP).
Lipids, represented by phospholipids, cholesterol, triglycerides (TG) and fatty acids, are considered essential to the human body, both by making up of the basic structure of cell membranes (phospholipids), and by acting as a precursor to steroid hormones, bile acids and vitamin D, as well as being a constituent of cell membranes, acting on the fluidity of the latter and in the activation of the enzymes located there (cholesterol)1. As for TG, these are formed from three fatty acids bound to a glycerol molecule and constitute one of the most important forms of energy storage in the body, and are deposited in the adipose and muscle tissue. In relation to lipoproteins, it is emphasized that these allow the solubilization and transport of lipids, usually hydrophobic substances, in aqueous plasma. It is important to note that there are four major classes of lipoproteins separated into two groups: a) those that are TG-rich, larger and less dense, represented by chylomicrons, of intestinal origin, and very low density lipoproteins, of hepatic origin, and b) those rich in cholesterol, forming low density (LDL-c) and high density (HDL-c) particles1. Coronary artery disease (CAD) has been delineated as the greatest epidemic humanity has ever faced.2 It takes a tremendous toll in premature sickness, disease, and death, which have a major economic impact on the person and upon the health care delivery system. Accounting nearly 80% of all cardiac morbidity, CAD is now the major cause of morbidity and mortality throughout the world. In most countries, it accounts for 30% of all deaths.3 Many studies demonstrate that atherosclerotic process has its silent beginning during childhood.4,5 The earliest grossly visible arterial lesions of the atherosclerotic process are Fatty streaks. Autopsy studies demonstrated that these fatty streaks are the precursors of mature atherosclerotic lesions.6 Dyslipidemia, hypertension, poor eating habits, sedentary lifestyle, constitute ideal conditions for the development of CAD. It is known that the pathology of atherosclerosis starts from childhood and if risk factors identified early and corrective steps are taken, the process can be delayed.7,8 For the primary prevention of coronary artery disease in adulthood, detection of dyslipidemia must begin early, followed by appropriate interventions to reduce it. Therefore, blood lipid profile in children should be screened as early as possible to detect dyslipidemia and management should involve the adoption of healthy lifestyles, reduction of total and saturated fat consumption and encouragement of physical activity. The present study would contribute to establish the norms of lipid profile in Indian children for which there are only a few studies from India9-13 In this context, the western norms may not be applicable for our setting in view of the divergent genetic, dietary, sociocultural and lifestyle factors.14
AIMS AND OBJECTIVE The present study was, designed to study lipid profile and prevalence of dyslipidemia among the university students in the age group of 19-21 years.
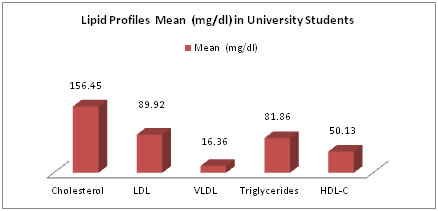
MATERIALS AND METHODS It was a descriptive and cross sectional study conducted over a period of 6 months (2017) on a sample of 126 conveniently selected first year medical university students between 19-20 years of age. Inclusion Criteria: Who were willing to take part in this programme Exclusion Criteria: previously diagnosed with diabetes, hypertension, hypothyroidism, nephrotic syndrome, or Dyslipidemia with and without treatment. Data collection procedure: The following parameters are measured for all the study subjects lipid profile. Laboratory investigations: Blood samples were collected from the antecubital vein, in the early morning, after a minimum of 12 hours of fasting period, in a supine position. Biochemical analysis Serum cholesterol, (TC) triglycerides (TG), Serum high density lipoprotein (HDL) were measured by International Federation of clinical chemistry (IFCC) approved enzymatic methods processed Autoanalyzer Erba- 200, reagents and calibrators were used for the analysis at medical college hospital laboratory, Vikarabad. Determination of VLDL And LDL Cholesterol was done by following Fried Ewald’s formula:22 VLDL Cholesterol (VLDL-C) = TG / 5 LDL Cholesterol (LDL-C) = TC - (HDL-C + VLDL-C) Normal Ranges: Cholesterol TC (mg/dl): Desirable<200, Borderline high risk, 200 – 239, High risk˃240. Serum triacylglycerol levels ( mg/dl), Normal Less than 150, Borderline high150 to 199, High 200 to 499, Very high˃500. LDL-C ( mg/dl): Optimal<100, Near optimal:100–129, Borderline High:130–159, High:160–189, Very High≥190. HDL-C: Serum HDL cholesterol: Low risk˃60, High risk<40. Preferred Cut -off Values: For serum lipids NCEP -ATP III Guidelines were used15. According to these standard guidelines, hypercholesterolemia is defined as TC >200mg/dl, LDL C as >100mg/dl, hypertriglyceridemia as TG >150mg/dl and HDL-C <40mg/dl. Dyslipidemia is defined by presence of one or more than one abnormal serum lipid concentration. Statistical Analysis: The data collected was analyzed statistically with the help of SPSS software (version 20.0) Continuous variables are expressed as mean±SD and percentile. Ethical Considerations: The study was approved by the ethics committee of the university. We obtained a written informed consent from all study subjects before enrolling them in the study. Confidentiality of data was preserved. OBSERVATIONS AND RESULTS The total participants were 126 healthy young students’ males and females admitted in first year private medical university students. Mean serum cholesterol in 126 students was 156.45+ 23.43 mg/dl, mean LDL-C was 89.92+ 22.73 mg/dl, mean VLDL 16.36+ 4.82 mean triglycerides were 81.86+ 24.08 mg/dl and mean HDL-C was 50.13+5.06 mg/dl. Table 1 and graph1
Table 1: Lipid Profile in University Students
Figure 1: DISCUSSION The elevated lipid profile is an important risk factor for cardiovascular diseases in among young adolescent population. The National Cholesterol Education Program (NCEP) recommends lipid screening beginning at age twenty and continuing every five years, with normal levels, and more frequently with abnormal levels throughout adulthood. This research provides information regarding the serum lipid levels among university students. Most of students were identified as having normal lipid levels. The balanced lipid profile is an important factor, in adolescent age to maintain good health and in the later life to avoid early morbidity. Thus blood lipid profiles in adolescents should be screened as early as possible to detect imbalances. In this study lipid profile norms and cut-off levels to define abnormalities for Indian adolescents were recommended NCEP. At the age of 19-21 years, the average Indian children enter graduation when the physical activity and dietary habits are likely to become better which may be the reason of lower TC, LDL-C, triglycerides and higher HDL-C levels observed in these adolescents.16 It is known that low HDL-C is an independent risk factor for CAD, not influenced by levels of LDL-C.17 In adults, the ratio of HDL-C to TC and HDL-C to LDLC are considered even more predictive for CVD.39 The TC/HDL-C ratio also called “atherogenic index” should ideally be around 5 and while the LDL-C/HDL-C ratio around 3.5. These have found a place as markers of coronary atherosclerosis.40 But have received limited attention in pediatric practice and studies. In our study, the mean atherogenic index (TC/HDL-C) was 3.1 and LDL-C/HDL-C ratio was 1.79. These correlate well to the TC/HDL-C ratio of 4.3±1.4 and LDL-C/HDLC ratio of 2.65±1.11 observed by Khalil et al.9 These ratios may find a use for risk assessment of atherosclerosis in adolescents in future.
Table 2: Similar studies
Health is a universal trait; the World Health Organization defines health as a “state of complete physical, mental, and social well-being, and not merely the absence of disease. Health contributes to general well-being and overall lifestyle. In order for a person to enjoy a quality of life, good health habits must be achieved because basic health determines what a person can do. Being a college student is basically a full-time job. It’s not always easy trying to balance classes with work, studying, social life, and of course health. A lot of students forget how important it is to maintain good health; it can affect whole college experience.
CONCLUSION The outcome of this study is most students attending this University, conduct a healthy lifestyle. Consuming a balanced diet, staying hydrated, and getting adequate amount of sleep, together with exercise and a healthy lifestyle will ensure both physical and mental health. It is recommended that children should have their lipid profiles checked at least by the age of 10 years, to detect imbalances early, so that necessary modifications in dietary consumption of fats, adoption of healthy lifestyles and encouragement of physical activity can be done.
REFERENCES
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.