 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 3 - March 2018
Serum uric acid, serum iron levels in normal pregnancy and preeclampsia patients
Rama Shouri1, Sarada Munagavalasa2*, Priyanka Vaitla3
1Associate Professor, Department of Biochemistry, RIMS, Adilabad, Telangana, INDIA. 2Assistant Professor, Modern Government Maternity Hospital, Hyderabad, Telanga, INDIA. 3Senior resident, Osmania Medical College, Hyderabad, Telangana, INDIA. Email: saradamunagavalasa1@gmail.com
Abstract Objective: Preeclampsia is pregnancy specific syndrome of reduced organ perfusion, secondary to vasospasm and endothelial activation associated with edema, BP: 140/90mm of Hg after 20 weeks of gestation and most frequently near term. Preeclampsia is the 3rd most common cause of maternal mortality constituting 6.8% of all pregnancies. Serum Uric Acid has a significant role in preeclampsia as a predictor marker, that it correlates well with preeclampsia as well as foetal out comes. The present study was conducted to assess the level of serum uric acid in preeclampsia patients and to see the relationship of serum uric acid levels with the fetal outcome. Methods: The study is conducted on 30 normal pregnant and100 preeclampsia patients between 24-34 weeks. Serum Iron levels and serum Uric acid levels are estimated in these patients. The data is analysed with prism statistics. Results: Serum Uric acid were found to be higher in preeclampsia patients compared to healthy control. Interpretations and Conclusion: Serum Uric Acid levels have an inverse relationship with the fetal outcome. Estimation of serum uric acid levels will be more useful screening test to predict Preeclampsia and also Foetal outcome Key Words: Preeclampsia, Serumuricacid, serumiron.
Preeclampsia is one of the most common cause of maternal and foetal morbidities and mortalities1. The pathological mechanism is characterized by a failure of the trophoblastic invasion of the spiral arteries leading to mal adaptation of maternal spiral arterioles which may be associated with an increased vascular resistance of the artery and decreased perfusion of placenta2,3. Hyperuricemia is believed to result from the decreased renal excretion that occurs as a consequence of the preeclampsia and also due to increased production, secondary to tissue ischemia and oxidative stress soluble uric Acid impairs nitric oxide generation in endothelial cells. Hyperuricemia induces endothelial dysfunction and may induce hypertension and vascular disease4. In this study there is significant role in S. Uric acid in developing hypertension. Hence Hyperuricemia is a early sensitive screening and diagnostic marker in PIH. Further Serum Iron are also estimated in the same preeclampsia and normal pregnant of same gestational age, there is decrease in Serum Iron levels5,6,7. Hence Serum Uric acid is simple and ideal screening and diagnostic test to predict Preeclampsia.
MATERIALS AND METHODS Study is conducted in two groups includes Group-I Includes 30 (n=30) healthy pregnant women aged between 20-30 yrs (controls) who were non diabetic, non hypertensive with no renal disease. Group-II comprises 100 (n=100) pregnant women with in the age group of 20-30 yrs with preeclampsia having BP>140/90mm of Hg and oedema being present. All Women in both the groups were in same gestational age (24-34weeks). 3ml of venous blood was collected in clean sterile bottle. Serum. Uric acid is estimated by phosphotungstic acid method. Serum Iron by Ferrozoine method. Serum Iron levels and serum Uric acid levels are estimated in these patients. The data is analysed with prism statistics.
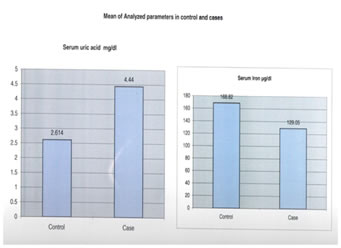
OBSERVATION AND RESULTS Mean value of controls of Serum Uric Acid is 2.61mg/dl and Serum iron 168.82µg/dl Mean value of Serum Uric acid of preeclampsia pts is 4.44mg/dl and Serum Iron of preeclampsia is 129.05µg/dl. There is significant increase in Serum Uric acid in Preeclampsia patients when compared with controls (p<0.001). Uric Acid is 4.44mg/dl. Serum Iron is 129.05mg/dl with cut off value being 2.83mg/dl for Uric acid, 140.9 for Serum Iron.. The sensitivity of Serum Uric Acid is 100%, specificity is 85% with diagnostic efficiency of 85% with regard to preeclampsia. The sensitivity of Serum Iron is 80% specificity is 100% with diagnostic efficiency of 85% with regard to Preeclampsia pts.
Table 1:
Figure 1:
The cut-off value is calculated by taking the mean of control and subtracting 2SD. The cut-off value of Serum Uric Acid is 2.83mg/dl with sensitivity 100% and Specificity 83.3, Diagnostic Efficiency 85%. The cut-off value of Serum Iron is taken 140.95µg/dl with sensitivity 80%, specificity 100%, Diagnostic Efficiency 85%
The cut-off value is calculated by taking the mean of control and subtracting 2SD. The cut-off value of Serum Uric Acid is 2.83mg/dl with sensitivity 100% and Specificity 83.3, Diagnostic Efficiency 85%. The cut-off value of Serum Iron is taken 140.95µg/dl with sensitivity 80%, specificity 100%, Diagnostic Efficiency 85%
Table 2:
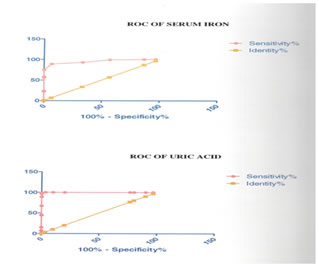
The best cut-off value is calculated by plotting ROC curves (Receiver operative curve)based on statistical Graff pad prism. The best cut-off value for Serum Uric acid is 3.45mg/dl with sensitivity 99%, Specificity 100%, Diagnostic efficiency 99%. The best cu-toff value for S. Iron is 150µg/dl with sensitivity 89%, specificity 93%, Diagnostic efficiency 92%
Table 3:
Table 4:
Figure 2:
DISCUSSION Preeclampsia is one of the largest cause of maternal and foetal mortality and morbidity. Hyperuricemia is often associated with Preeclampsia1. In Normal pregnancy there is alteration in GFR and ERPF (effective renal plasma flow). In PIH there is vasospastic involvement of Kidney and Placenta9. In kidney the renal tubular damage preceeds to the glomular impairment10 so the secretary capacity of the renal tubule is effected first. The plasma is full of trophoblastic tissues which are very rich in Purines, as pathological process of Toxaemia of Pregnancy. conglomeration of trophoblastic tissues is placenta and its vasospastic disorder results in degeneration of Purines thus producing much Uric Acid. Uric Acid has recently been to shown to reduce endothelial nitric oxide bioavailability and to inhibit endothelial proliferation11,12. As maternal Uric Acid passes freely into the placenta, a rise in Uric Acid could lead to inhibition of foetal angiogenesis in the third trimester, which might lead not only to a small infant but also to the inhibition of kidney growth with a reduction in nephron number11,13. Uric acid is simple supportive measure used to confirm the diagnosis of Preeclampsia to one in which we appreciate its independent link with adverse out comes. It is reasonable to incorporate the measurement of Serum Uric acid in the standard assessment of women with hypertension in Pregnancy. The major stores of Iron are located in RBC and Liver. Elevated Serum Iron levels observed in many patients with preeclampsia is derived from large part of Haemolysis5. Haemolysis is due physical destruction of RBC as a result of intense vasospasm on abnormal endothelial cells erythrocyte interaction. According to other studies also, levels have been shown to be increased in pts with preeclampsia6,7,5. There are also other studies in which Serum Iron concentration decreases gradually during Pregnancy8. Normally both Serum Iron and Ferritin show a decrease with advancing gestation due to hemodilution and depletion of Iron stores to meet the increasing needs of the growing conceptus14. In the present study also there is decrease in Serum Iron Levels during Preeclampsia
CONCLUSION It is clear from the results of the present study that there is a significant association between hyperuricemia and preeclampsia. Though we recommend further studies in this regard, we suggest that the level of Uric Acid is to be considered as predicting factor of preeclampsia during first evaluation, and also should be checked at every month and recorded, so that, preventive measures can be taken for both mother and fetalout come. REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.