 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 3 - March 2018
Study of association between Hypothyroidism and kidney dysfunction
Sowjanya Yerram1, Bhanupriya Tammineni2*
1Assistant Professor, Department of Biochemistry, NRI Medical College, Chinakakani, Guntur, Andhra Pradesh, INDIA. 2Assistant Professor, Department of Biochemistry, ASRAM medical college, Eluru, West Godavari, Andhra Pradesh 534005, INDIA. Email: drsowji85@gmail.com, bhanu.tammineni@gmail.com
Abstract Thyroid hormones have a significant impact on kidney health and disease. Thyroid hormones have pre-renal and intrinsic renal effects by which they increase the renal blood flow and Glomerular filtration rate. Several studies indicate that thyroid hormones directly influence normal growth, development and physiology of kidneys. Hypothyroidism is associated with reduced GFR, increased serum Creatinine and blood Urea levels indicating renal dysfunction with several molecular and hemodynamic factors regulated by thyroid hormones. The purpose of this study was to screen for renal disease in hypothyroid patients and to find association between kidney dysfunction and hypothyroidism. A study on RFT (serum creatinine and blood urea levels) in newly diagnosed 40 hypothyroidism patients attended OPD over a period of 4 months and 40 age and sex matched healthy controls was done. The statistical analysis of serum T3 (P<0.001), T4 (P<0.001), TSH (P<0.001), Urea (P<0.001) and serum creatinine (P<0.001) were highly significant indicating significant association between kidney dysfunction and thyroid profile. There is a consistent and reversible increase of serum creatinine and Urea levels in the hypothyroid state. Most of the renal manifestations of thyroid disorders, which are clinically most significant with Hypothyroidism, are reversible with treatment and this study needs further evaluation. Key Words: Hypothyroidism, Glomerular filtration rate, Kidney dysfunction, Serum Creatinine.
Thyroid hormones (TH) are necessary for normal growth, development and physiology of kidneys. They are also involved in maintenance of water and electrolyte homeostasis in different organs and tissue departments.1 Thyroid hormones have pre-renal and intrinsic renal effects by which they increase the renal blood flow and Glomerular filtration rate (GFR)2,3.
Effects of Thyroid Hormones on Renal Physiology
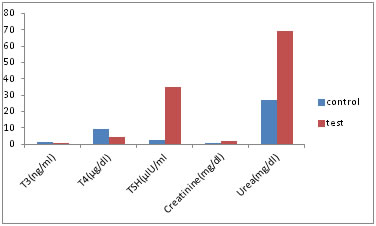
Thyroid dysfunction causes significant changes in kidney function. Primary hypothyroidism is associated with a reversible elevation of serum creatinine in both adults4,5 and children6,7. This increase is observed in more than half (~55%) of adults with hypothyroidism. It is associated with a reduction of GFR and RPF that are normalized following levothyroxine administration. Normalization of circulating TH concentrations with replacement therapy in hypothyroid patients with chronic kidney disease (CKD) can significantly improve GFR8. Hypothyroidism is often accompanied with decline of kidney function, or failure of electrolyte balance. The decline of kidney function is accompanied by changes in the synthesis, secretion, metabolism and elimination of TH9. MATERIALS AND METHODS A study on serum creatinine and blood urea levels in newly diagnosed hypothyroid patients attended OPD at NRI General and Super Speciality Hospital, Chinnakakani was done. Inclusion Criteria: 40 age and sex matched healthy individuals as control group and 40 Hypothyroid patients as test group between the age of 20-50 yrs were taken. Exclusion Criteria: Cases with Hypertension, Diabetes Mellitus, Liver diseases, kidney diseases, children, pregnant women and elderly aged were excluded from the study. Sampling and Data collection: Each patient’s written informed consent was taken to participate in the study. The following investigations were carried out on the study subjects like Serum T3, T4, TSH, creatinine and urea levels were estimated. Plain vacutainer was used. The samples were separated by centrifugation at 2400 rpm. Serum Creatinine (Alkaline picrate Method) and Urea (Urease kinetic Method) were analyzed in DADE Dimension automated system. Thyroid profile (T3, T4, TSH) was estimated by Automated Electro Chemiluminescence (ECLIA) method using commercially available kit by ROCHE Cobas e411 For adequate quality control both normal, abnormal reference control serum solutions and calibrators were run before each batch. Other factors influencing the quality, like proper functioning of instrument, temperature, glassware, cuvettes, distilled water were taken care. RESULTS Data evaluation was done using SPSS software. The results were expressed as mean (standard deviation). The P value was used to compare the different groups. The P value <0.05 was considered significant. The mean and standard deviation of biochemical characteristics of the two groups were calculated. The statistical analysis of serum TT3 (P<0.001), TT4 (P<0.001), TSH (P<0.001), Urea (P<0.001) and Creatinine (P<0.001) by Student t test were highly significant indicating significant association between kidney dysfunction and Hypothyroidism.
Table 1: Showing biochemical parameters between control and test group
hs – highly significant
Figure 1: Comparision of biochemical parameters between control and test group
DISCUSSION Thyroid dysfunction affects renal physiology and development, whereas kidney disease could result in thyroid dysfunction. Disorders of the thyroid and kidney may co-exist with common etiological factors. The most common kidney derangements associated with hypothyroidism are an increase in serum creatinine levels, reduction in GFR and renal plasma flow, decreased capacity of free water excretion and hyponatremia10. Montenegro et al11 showed a decrease in glomerular filtration rate (GFR) in all of their hypothyroid patients, whereas only 55% had an increase in serum creatinine levels. Villabona et al12 described the decrease in effective renal blood flow and GFR in hypothyroid patients with chronic renal disease. Stuart H Kreisman et al4 found that serum creatinine levels were 35% higher in the hypothyroid state. Our study showed that 63% had an increase in serum creatinine levels in hypothyroid patients. Hypothyroidism results in a reversible elevation in serum creatinine due to the reduction in GFR as well as possible myopathy and rhabdomyolysis. Although the exact mechanism of these changes has not been defined yet, it seems that kidney failure secondary to hypothyroidism involves heterogenous processes based on the direct or indirect effects of thyroid hormones on renal hemodynamics13,14 Thyroid hormone deficiency decreases myocardial contractility and cardiac output. On the other hand, an impaired endothelial-mediated vasodilatation in hypothyroidism increases peripheral and renal vascular resistance(14). These effects reduce renal plasma flow and GFR, resulting in free water overload and decrease in creatinine clearance. Consequently, elevation of plasma creatinine levels might happen. Whilst the pathophysiology of impaired renal function in hypothyroidism is multifactorial, the reduction in GFR due to the lower cardiac output and renal blood flow is likely to be the predominant mechanism1 It has also been suggested that thyroxine may mediate tubular secretion of creatinine(15). Furthermore, hypothyroidismmay increase creatinine release from muscle16. Although freely filtered, additional tubular secretion of creatinine renders it a poor marker of GFR. There are some published reports confirming stabilisation of kidney function in patients with chronic kidney disease after correction of thyroid function17,18. There are also described cases of acute deterioration of kidney function in patients with chronic kidney disease and unrecognised hypothyroidism19. We therefore recommend measurement of serum thyrotropin and thyroxin levels in all cases of renal failure with undefined renal disease, even if the typical clinical presentation of hypothyroidism is absent. We also recommend that thyroid hormone assays should be performed in all patients with chronic kidney disease whose kidney function is rapidly worsening.
CONCLUSION There is a consistent and reversible increase of serum creatinine in the hypothyroid state, presumably due to a decrease in the GFR. Most of the renal manifestations of thyroid disorders, which are clinically most significant with hypothyroidism, are reversible with treatment. The presence of reversal renal failure as the consequence of hypothyroidism is usually subtle and frequently overlooked. Knowledge of the association between hypothyroidism and deterioration of renal function is very important in clinical practice. This association must be recognized in time, avoiding the unnecessary diagnostic procedures that postpone adequate treatment.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.