 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 8 Issue 1 - October 2018
Prevalence of metabolic syndrome and its components among young adults at a tertiary care hospital in Puducherry
Suryapriya Rajendran1, Manju M2*, Ajai Premkumar3, Sasmita Mishra4
1Assistant Professor, 2Associate Professor, 3Second year MBBS Student, 4Professor and HOD, Department of Biochemistry, Aarupadai Veedu Medical College and Hospital, Puducherry, INDIA. Email: drmanjumay1@gmail.com
Abstract Background: Metabolic syndrome refers to a group of risk factors that increase the risk for the development of type 2 diabetes mellitus and cardiovascular diseases. The prevalence of metabolic syndrome is increasing worldwide and the prevalence varies with age, gender and race. Objectives: To estimate the prevalence of metabolic syndrome among young adults at a tertiary care hospital in Puducherry. Materials and Methods: Three hundred young adults (150 men and 150 women) of 20-40 years of age were recruited. Metabolic syndrome was defined as per modified NCEP-ATP III guidelines with modification of waist circumference applicable to South Asians. Results: The prevalence of metabolic syndrome was 25% among young adults (27.3% in men and 22.7% in women). Waist circumference was the most prevalent component in both men and women. Low HDL cholesterol was the second most prevalent component in both men and women, with women having significantly higher prevalence than men. The prevalence of elevated triglyceride was significantly higher in men, compared to women. Conclusion: High prevalence of metabolic syndrome among young adults, suggests that these young adults have higher risk of developing type 2 diabetes mellitus and cardiovascular disease in later life. Hence, periodic screening can be done for early diagnosis of metabolic syndrome among young adults and life style modifications can be initiated at an earlier age to prevent the development of type 2 diabetes mellitus and cardiovascular diseases. Key Words: Metabolic syndrome, Prevalence, Puducherry, Young adults.
Metabolic syndrome refers to a cluster of risk factors that increase the risk for the development of type 2 diabetes mellitus and cardiovascular diseases. This syndrome is characterized by central obesity, glucose intolerance, hypertension and dyslipidemia.1-2 There are several criteria for defining metabolic syndrome, but the commonly used criteria include Adult Treatment Panel III and adapted Adult Treatment Panel III by the National Cholesterol Education Programme, International Diabetes Federation criteria and the World Health Organization criteria.3 Metabolic syndrome is a growing public health problem worldwide, affecting one-fourth of the adult population.4 The prevalence also varies with age, gender and race.5 The risk factors that lead to metabolic syndrome are sedentary life style, physical inactivity, poor dietary pattern and abdominal obesity. These factors increase predisposition towards metabolic syndrome, when they occur at an early age.6 Though the risk for cardiovascular disease is low among young adults, these risk factors may continue to act even in their adulthood leading to these diseases in their later life. So, early identification of metabolic syndrome among young adults can help in preventing the development of diseases associated with this syndrome.5 At present, there are no published data available on the prevalence of metabolic syndrome among young adults in Puducherry. Hence, the present study was aimed to estimate the prevalence of metabolic syndrome and its components among young adults at a tertiary care hospital in Puducherry.
MATERIALS AND METHODS Study design and population: The study was a hospital based cross-sectional study conducted in the Department of Biochemistry, Aarupadai Veedu Medical College and Hospital, Puducherry, India. The study was approved by our Institutional Research Committee and Ethics Committee (human studies). 300 young adults (150 men and 150 women) of 20-40 years of age were recruited after getting written informed consent from them. The study subjects were selected by consecutive sampling method from patients attending the master health check up of Aarupadai Veedu Medical College and Hospital, Puducherry. People with liver diseases, renal diseases, inflammatory diseases, vascular diseases, endocrine diseases and cancers were excluded from the study. Data Collection: A detailed clinical history was collected from the study subjects through a pre-tested, semi-structured questionnaire. Height and weight was measured and body mass index (BMI) was calculated by the formula: weight in kg/ height in m2. Waist circumference was measured at mid-way between the iliac crest and the last rib. Blood pressure was measured in right arm in sitting position using standard mercury sphygmomanometer. 3mL of fasting venous blood sample was collected. Fasting blood glucose, serum triglyceride and HDL cholesterol was assayed in the fully automated biochemistry analyzer (Mindray BS-380). Fasting blood glucose was measured by glucose oxidase – peroxidase method using reagent kits from Jeev diagnostics private limited, Chennai, Tamil Nadu, India. Serum triglyceride was estimated by glycerokinase peroxidase – peroxidase method and HDL cholesterol was estimated by direct method using reagent kits from Shenzhen Mindray bio-medical electronics co limited, China. Definition of metabolic syndrome: Metabolic syndrome was defined according to the modified NCEP- ATP III guidelines with modification of waist circumference that is specifically applicable to South Asians.7 The study subjects were diagnosed to have metabolic syndrome if 3 out of the following 5 criteria are present: 1) elevated waist circumference ≥ 90cms in men and ≥ 80cms in women, 2) elevated blood pressure ( ≥ 130/85 mm Hg), 3) elevated fasting blood glucose ≥ 100 mg/dL or drug treatment for diabetes mellitus, 4) elevated serum triglyceride ≥ 150mg/dL, 5) reduced serum HDL ≤ 40mg/dl in men and ≤ 50mg/dl in women. Statistical Analysis: Normally distributed variables are expressed as mean with standard deviation and non-normally distributed variables are expressed as median (interquartile range). Prevalence of metabolic syndrome was calculated by using the formula: Prevalence = (No. of cases of metabolic syndrome / No. of subjects studied) ×100. Prevalence is expressed as percentage. Prevalence of metabolic syndrome and its components was compared among men and women by using chi square test. Comparison of anthropometric variables and components of metabolic syndrome among men and women was assessed by student’s unpaired t test (for normal data) or Mann Whitney U test (for non-normal data). A p value of <0.05 was considered as statistically significant. All the statistical analysis were performed by using SPSS software version 16 (SPSS Inc., USA). RESULTS A total of 300 young adults of age 20-40 years (150 men and 150 women) were included in the study. Comparison of characteristics among men and women are shown in Table 1. No significant difference was found between men and women in age, body mass index, systolic blood pressure, diastolic blood pressure and fasting blood glucose. Height, weight, waist circumference and serum triglyceride levels were significantly higher in men compared to women. HDL cholesterol levels were significantly low in men compared to women.
Table 1: Comparison of characteristics among men and women
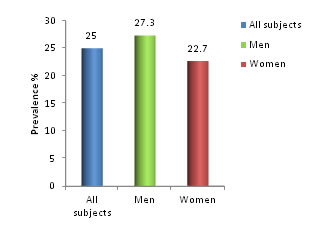
Values are expressed as mean±SD; Serum TGL expressed as median (interquartile range);a p value<0.05, statistically significant between men and women. The prevalence of metabolic syndrome among young adults is shown in Figure 1. The prevalence of metabolic syndrome among young adults was 25%. The prevalence was higher in men (27.3%) compared to women (22.7%), but this difference was not statistically significant.
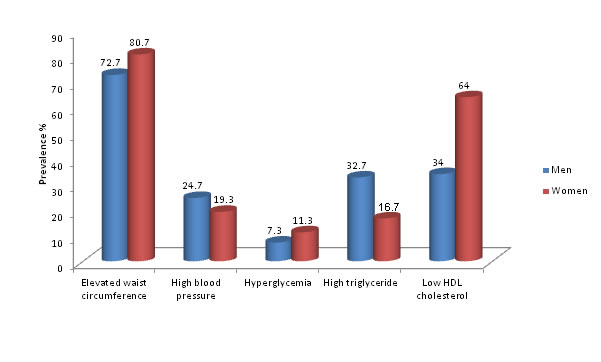
Then the prevalence of individual components of metabolic syndrome among men and women is shown in Figure 2. Among men, the most frequent component of metabolic syndrome was elevated waist circumference (72.7%), followed by low HDL cholesterol (34%), followed by high triglyceride levels (32.7%), followed by high blood pressure (24.7%) and the least component was high fasting blood glucose levels (7.3%) Among women, the most prevalent component was elevated waist circumference (80.7%), followed by low HDL cholesterol (64%), followed by high blood pressure (19.3%), followed by high triglyceride levels (16.7%) and the least component was high fasting blood glucose levels (11.3%). The prevalence of low HDL cholesterol and high triglyceride levels was statistically significant between men and women with p value of <0.001 and 0.001 respectively. There was no statistically significant difference in the prevalence of other components of metabolic syndrome between men and women.
Figure 2: Comparison of prevalence of components of metabolic syndrome among young adult men and women
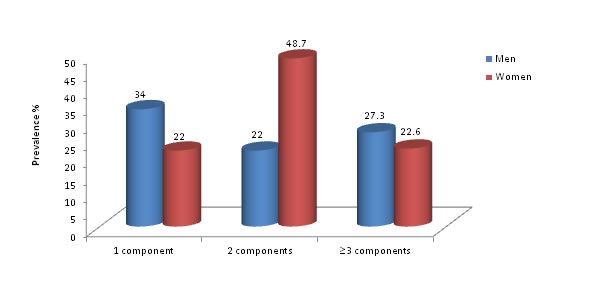
Figure 3 shows the prevalence of number of components of metabolic syndrome in men and women. In men, 34% had one component, 22% had two components and 27.3% had three or more than three components. In women, 22% had one component, 48.7% had two components and 22.6% had three or more than three components. The prevalence of one component was significantly higher in men compared to women with a p value of 0.028, whereas the prevalence of two components was significantly higher in women compared to men with a p value of <0.001.
Figure 3: Comparison of prevalence of number of components of metabolic syndrome among young adult men and women DISCUSSION Metabolic syndrome is defined as a cluster of risk factors associated with diabetes mellitus and increased risk for cardiovascular diseases.8 It is caused by the involvement of various factors such as stress, metabolic, genetic and environmental factors. Since metabolic syndrome can lead to cardiovascular disease, diabetes mellitus, asthma and some cancers, it is essential to estimate the prevalence of metabolic syndrome in population of various regions.3 The health condition of young adults becomes more important in developing countries, as they contribute much to the workforce of a country.9 Hence, the present cross-sectional study was done to estimate the prevalence of metabolic syndrome among young adults at a tertiary care hospital in Puducherry. The prevalence of metabolic syndrome among young adults was found to be 25%, with the higher prevalence in men (27.3%) than women (22.7%). Similar results were observed in a study conducted by Chow et al,10 in rural Andhra Pradesh among adults, which showed a prevalence of 24.6%, with higher prevalence in men (28.6%) compared to women (20.4%). In another study conducted in north India among young adults, the prevalence was 22.47%, which was similar to the present study but they showed higher prevalence in women.11 This gender difference can be due to difference in their hormone levels and sex binding globulin levels.12 Among the five components of metabolic syndrome, elevated waist circumference was the most prevalent component found in young adults, in both men and women. This is consistent with the findings observed in many studies conducted in different age groups and gender in Kerala, Tamil Nadu and Ecuador.13-15 Central obesity was also the most prevalent component of metabolic syndrome in ‘Young adult health in Saudi Arabia’ study16 and also in a study conducted in Korean young adults.17 In the present study, 72.7% of men and 80.7% of women had elevated waist circumference, which is an indirect measure of visceral fat accumulation. This increased prevalence of obesity among young adults can be due to change in their dietary patterns and life style habits like increased usage of electronic gadgets. These changes lead to increased body mass index and central obesity by affecting our body composition and metabolism.18 Central obesity is considered to be one of the chief features of metabolic syndrome, because of elevated plasma free fatty acid levels and peripheral insulin resistance.19 Central obesity characterized by android type of fat deposition is found to be an independent risk factor for cardiovascular disease20 Low HDL cholesterol was found to be the second most prevalent component in both men and women, with prevalence being significantly higher in women (64%) than men (34%). A study conducted in Kerala, also showed significantly high prevalence of low HDL cholesterol in women (70.4%) compared to men (37%). Similar findings have been seen in other studies conducted across south Asia.13 The third and fourth prevalent components showed differences according to the gender. In men, high triglyceride levels was more prevalent than elevated blood pressure while in women, elevated blood pressure was more prevalent than high triglyceride levels. In Young Finns Study21 conducted among young adults, hypertriglyceridemia was more prevalent in men than women, similar to our findings. Dyslipidemia, found in metabolic syndrome is mostly due to increased release of free fatty acids from adipocytes. These fatty acids increase the concentration of plasma LDL cholesterol and VLDL cholesterol by increasing the synthesis of cholesterol, triglyceride and apoproteins. Then cholesterol ester transfer protein exchanges core lipids in these lipoproteins and cause increased production of small dense LDL cholesterol, the important feature of atherogenic dyslipidemia.18 Dyslipidemia, characterized by high triglyceride and low HDL cholesterol levels, is found to be the key feature of insulin resistance. Both high triglyceride and low HDL cholesterol were found to be better predictors of type 2 diabetes mellitus.20 In our study, the least component of metabolic syndrome in both men and women was impaired fasting blood glucose levels. A study conducted among young adults in Turkey,20 also found fasting blood glucose as least component in both men and women. In this study, we found that men had a significantly higher prevalence of one component of metabolic syndrome, whereas women had a significantly high prevalence of two components. Preventive measures have to be started at a very early stage, even when one component of metabolic syndrome is found, in order to prevent the development of the three components, required for diagnosing metabolic syndrome.22 Metabolic syndrome has a greater risk of cardiovascular disease mortality compared to the risk associated with the individual components of metabolic syndrome. Hence the young adults with collection of metabolic syndrome components have to be targeted for primary prevention.23
CONCLUSION The prevalence of metabolic syndrome among young adults is 25%. High prevalence of metabolic syndrome among young adults, suggests that these young adults have higher risk of developing type 2 diabetes mellitus and cardiovascular disease in later life. Hence, metabolic syndrome has to be prevented by promoting healthy life style among young adults. Healthy life style includes changing their dietary habits such as increasing the consumption of vegetables, fruits, whole grains, proteins, monounsaturated and polyunsaturated fatty acids, restricting the intake of saturated fat and trans-fatty acids and increasing physical activity by doing aerobic exercises.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.