 Home
Home|
Table of Content Volume 4 Issue 2 -November 2017
Unusual trifurcation of brachial artery, superficial course of ulnar artery and absence of palmaris longus muscle: A case report
Bangale Sridevi P
Junior Resident, Department of Anatomy, Government Medical College, Latur, Maharashtra, INDIA. Email: drsridevibangale@gmail.com
Abstract During routine dissection for undergraduates in department of anatomy, Seth G. S. M. C. Mumbai, a unilateral case of trifurcation of brachial artery into radial, ulnar and common interosseous artery in a adult male cadaver in his right upper limb was found. In same limb, the ulnar artery was superficial which was anastomosing with the superficial palmar branch of the radial artery, creating the superficial palmar arch and absence of Palmaris longus muscle in same limb was observed. Trifurcation of brachial artery into radial, ulnar and common interosseousarteries is common variation. Though ulnar arterial variations are rare, superficial ulnar artery is one of its commonest variations. The arterial variations of upper limb are useful for vascular surgeons, interventional radiologists, plastic surgeons and clinicians. Absence of palmaris longus muscle is also a common variation. It is of intrest in orthopaedic, hand and reconstructive surgeries. Key Words: Brachial, Superficial, ulnar, Palmaris longus, radial, variation.
The arterial variations of upper limb are useful for vascular surgeons, interventional radiologists, plastic surgeons and clinicians. An intimate knowledge of arterial anatomy of upper extremities and its common variations is indispensable to limb surgeons. Appreciation of variations in the upper extremity vasculature is essential to prevent injury, thrombosis, gangrene and even amputation of limbs, particularly in patients requiring dialysis or undergoing arteriography. For both surgical and routine patients, an accurate knowledge of course and relations to surrounding structures is of great Importance. The brachial artery is a continuation of axillary artery, at the distal border of teres major. It runs in the anterior compartment of the arm to enter the cubital fossa and ends at the level of neck of radius by dividing into radial and ulnar arteries to supply the forearm and hand. The ulnar artery passes medially deep to the pronator teres muscle and then runs to the distal part of the forearm together with the ulnar nerve.1 Superficial ulnar artery is a rare variation of the ulnar artery. It usually arises higher up, either in the axilla or the arm and runs a superficial course in the forearm before entering the hand.2 Palmaris longus (PL) is one of the most variable and most superficial flexor muscles of the forearm. It is well known that there is a wide variation in the reported prevalence of PL absence in different ethnic groups.3 Although the function is very less, PL receives the attraction of the surgeons for its use in reconstructive plastic and hand surgery as tendon graft, in lip augmentation or escalation,4 ptosis correction5 and also in some facial paralysis management6. I hereby report a case of trifurcation of brachial artery into radial, ulnar and common interosseous arteries at neck of radius. Superficial ulnar artery (SUA), then runs superficially in the forearm to reach the palm. In the same forearm, absence of Palmaris longus muscle also noted.
CASE REPORT During routine dissection of upper limb for undergraduates teaching in the Department of Anatomy, Seth G. S. medical college, mumbai, abnormal trifurcation of brachial artery into radial, ulnar and common interosseous arteries was observed in right upper limb of a adult male human cadaver. (fig. no. 1). Superficial course of ulnar artery was observed in same cadaver. (fig. no. 2). The ulnar artery (superficial ulnar artery) originated from the brachial artery descended in a superficial plane deep to antibrachial fascia. In the forearm, the ulnar artery descended in front of common tendinous origin of superficial forearm flexors from the medial epicondyle, but just deep to the bicipital aponeurosis. Then it descended on medial aspect of front of the forearm, superficial to pronator teres, flexor carpi radialis and flexor digitorum superficialis. Just proximal to the flexor retinaculum, it was accompanied by the ulnar nerve on its medial side with which it descended superficial to flexor retinaculum through Gyon’s canal, to reach the palm. In the palm, after giving a deep branch, it continued as superficial palmar arch. In its course through the forearm, the ulnar artery gave branches to the muscles and skin. But it failed to give anterior ulnar recurrent, posterior ulnar recurrent, palmar carpal and dorsal carpal branches. Also absence of Palmaris longus muscle was observed in same right forearm. (fig. no. 3)
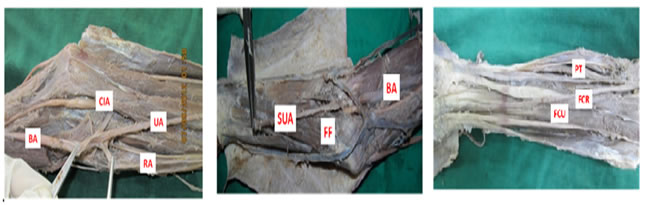
Figure 1: Trifurcation of brachial (BA) artery into radial (RA), ulnar (UA) and common interosseous arteries (CIA) Figure 2: Superficial course of ulnar artery in forearm. SUA- superficial ulnar artery, FF- forearm flexors, BA- brachial artery Figure 3: Absence of palmaris longus muscle. PT- pronator teres, FCR- flexor carpi radialis, FCU- flexor carpi ulnaris DISCUSSION William et al (1999)1 have mentioned that the brachial artery may bifurcate proximally and reunite to form single trunk. It sometimes, trifurcate proximally into ulnar, radial, and common interosseous arteries. Huber (1930)7 observed trifurcation of brachial artery into ulnar, radial, common interosseous arteries or median artery. Patnaik et al (2001) 8 have found trifurcation of brachial artery into ulnar, radial, and radial recurrent arteries in a right superior extremity of fifty years old male cadaver during dissection. Third branch was radial recurrent artery. While common interosseous artery was given off from the ulnar artery, which divided into anterior and posterior interosseous arteries, the radial artery passes normally to its destination. Henry Hollinshed (1962)9 has stated that ‘‘one of the two arteries lie superficial to superficial flexor group of muscles. The other artery is taking the usual course is crossed superficially by the median nerve’’. Ulnar artery is present superficial to superficial flexor group of muscles in approximately 3% of the populations, and then the artery may be pulsatile or visible.10 Knowledge of origin, course and distribution of ulnar artery is important due to its clinical implications. The incidence of the superficial ulnar artery arising from the axillary artery varies between 0.7% and 2%.11 In present study trifurcation of brachial artery into ulnar, radial and common interosseous arteries in right upper limb was seen and same upper limb of same body showed ulnar artery running superficial to superficial flexor group of muscles, whereas radial artery was running its usual course. The superficial ulnar artery may be associated with the absence of the palmaris longus muscle. The development and clinical significance of superficial ulnar artery has also been reported by Reddy and Vollala.12 Most standard textbooks of hand surgery quote the prevalence of absence of palmaris longus at around 15%. However, this figure varies considerably in different ethnic groups.13,14
CONCLUSION The above variations of brachial artery is common rather an exception. These variations are not explained in any conventional text book. But still, this particular knowledge of above variations is found to have clinical importance especially in the field of vascular surgery.15 Knowledge of above unusual pattern of brachial artery is important clinically, in order to avoid accidental injuries or intra-arterial injections, arterial grafts for coronary bypass, flap sugery and in vascular surgery. A superficial ulnar artery may complicate intravenous drug administration, venipuncture, and percutaneous brachial catheterization. Superficial course of ulnar artery from the middle of the arm till distal part of the forearm makes it vulnerable for injuries. Any superficial cut might result in severe bleeding. Knowledge of this variation is very important to radiologists, orthopedic and plastic surgeons for appropriately planning the operative procedures.16 Palmaris longus is considered to be a dispensable tendon because its absence does not significantly affect the function of the wrist. It is therefore very useful in orthopaedic, hand and reconstructive surgery. It is commonly used by hand surgeons for tendon transfers, second stage tendon reconstruction, pulley reconstruction as well as tendon grafts. Plastic surgeons also utilise the palmaris longus in restoration of lip and chin defects.17
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.