 Home
Home|
Table of Content Volume 11 Issue 1 - July 2019
Morphometric analysis of dry human mandibles - Application in inferior alveolar nerve block
Alka Bhingardeo1, Mehera Bhoir2*
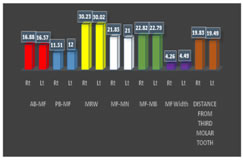
1Registrar, 2Professor & HOD, Department of Anatomy, HBTMC & Dr. R. N. Cooper Mun. Gen. Hospital Mumbai, Maharashtra, INDIA. Email: dr.alkabhingardeo@gmail.com Abstract Background: Mandible is the strongest bone of the face which is preferred after pelvis for sex determination by forensic experts. In case of inferior alveolar nerve block, given in various maxillofacial surgery, the nerve is to be anesthetized at the level of mandibular foramen by Halsted approach. The reason for high failure rate of mandibular nerve block is the variations in the location of mandibular foramen. So the knowledge of morphometry of mandibular ramus and mandibular foramen will help in accurate localization of foramen and help in preventing complications like haemorrhage, injury to the neurovascular bundle, fractures and necrosis of mandibular ramus. Materials and method: The study was carried out on 86 dry human mandibles. The distance of mandibular foramen from the different borders of ramus and from the third molar tooth were measured with the help of Digital Vernier calliper. The presence of accessory mandibular foramen was also noted. Results: Results of morphometric parameters of ramus were - AB-MF(RT)-16.88, AB-MF(LT)-16.57, PB-MF(RT)-11.51, PB-MF(LT)-12, MF-MN(RT)21.85, MF-MN(LT)-21, MF-MB(RT)-22.82, MF-MB(LT)-22.79, MRW(RT)-30.23 and MRW(LT)-30.02 mm. Incidence of accessory mandibular foramen was 42.68%. Mean diameter of mandibular foramen was 4.26 mm on the right side while 4.49 mm on the left side. Conclusion: There were variations in the different morphometric parameters of mandibular ramus and in the location of mandibular foramen. Knowledge of such variations will be helpful to the maxillofacial surgeons, forensic experts, radiotherapist in radiotherapy of tumours of maxillofacial region and anatomists. Key Word: mandible, mandibular foramen, inferior alveolar nerve block
INTRODUCTION Mandible is the longest, strongest and lowest bone of the face.1 It develops from the first pharyngeal arch cartilage - Meckel’s cartilage.2 In the newborn, the body of the mandible is composed of two halves which are united by a fibrous tissue. This is replaced by bone after two years. Mandible is having body and two oblong rami. Ramus is a quadrilateral plate with two surfaces and four borders. The surfaces are- medial and lateral while borders are –superior, inferior, anterior and posterior. On the medial surface of each ramus mandibular foramen is located. It is located a little above the medial surface of mandible. The foramen leads to mandibular canal within the body of mandible. The foramen transmits inferior alveolar nerve and vessels. Inferior alveolar nerve is the branch of posterior division of mandibular nerve. It enters the mandibular foramen and travels though mandibular canal. Before entering into the foramen, it gives mylohyoid branch. Inside the mandibular canal, it divides into incisive and mental branches and supplies teeth, gingivae and upper lip.1,3 In case of inferior alveolar nerve block, the nerve is to be anesthetized at the level of mandibular foramen by Halsted approach. Malamed reported that this approach is successful in 80-85% of patients. So the accurate location of mandibular foramen is mandatory. The failure rate of inferior alveolar nerve block is 20-25%. The reason for this high failure rate is the variations in the location of mandibular foramen. Variations are produced due to difference in relative development of muscles of mastication leading to variations in the ramus morphometry. 4 Failure of block is also due to occasional presence of accessory mandibular foramina. Accessory mandibular foramen may be single or many. It transmits extra branches of inferior alveolar nerve. It can transmit auxiliary nerves (from facial, mylohyoid, buccal, transverse cervical cutaneous and other nerves).1 Missing of such foramina leads to inadequate anesthetization of inferior alveolar nerve. The complications of inferior alveolar nerve block are haemorrhage, injury to the neurovascular bundle, fractures and necrosis of mandibular ramus.5 So accurate localization of morphometry of mandibular ramus with precise localization of mandibular and accessory mandibular foramen is essential. This knowledge is useful for anatomist, maxillofacial surgeons and forensic experts.6Accessory foramen has also been found to spread tumor cells following radiotherapy on the lateral surface of mandible. The knowledge of accessory mandibular foramen is also useful for radiotherapist for planning radiation therapy in the lateral mandibular region.5The ramus is also related with other nerves- the masseteric nerves, auriculotemporal nerve and lingual nerve.1 So the knowledge of the morphometry of ramus is not only useful for localization of mandibular and accessory mandibular foramen but also in various surgeries of maxillofacial region in order to avoid damage to these nerves.
MATERIALS AND METHOD The study was carried out on 86 dry human mandibles. Dry human mandibles were procured from the tertiary health care centres of Mumbai. Mandibles with fracture, trauma or eruption were excluded from the study. The different measurements of ramus of mandible were measured with the help of Electronic sliding digital Vernier calliper with resolution of 0.02 both on right and left side. Various measurements taken were as follows- AB-MF-distance of mandibular foramen from the anterior border. PB- MF-distance of mandibular foramen from the posterior border. MRW- it is minimum anteroposterior breadth of ramus measured at the level of mandibular foramen. MF- MN- distance of mandibular foramen from the mandibular notch. MF-MB–distance of mandibular foramen from the inferior border of mandible. Diameter of mandibular foramen and Distance of mandibular foramen from the third molar tooth were measured by Vernier calliper. Presence of accessory mandibular foramen was noted. OBSERVATIONS AND RESULTS Table 1: statistical analysis of various parameters of ramus morphometry in relation to the mandibular foramen
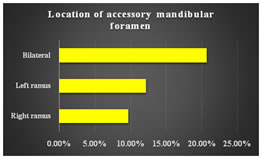
Graph 1 Graph 2 Graph 1: showing Mean values of different parameters of mandibular ramus on right and left side; Graph 2: Location of accessory mandibular foramen
Table 2: incidence of mandibular foramen at different locations
Table 3: showing Mean values of different parameters of mandibular ramus on right and left side in different studies
Table 4: Minimum ramus width (MRW) in different studies
Table 5: Incidence of Accessory mandibular foramen in different studies
DISCUSSION The mandibular foramen is present on the medial surface of the ramus of mandible. So the knowledge of morphometry of ramus and the distance of mandibular foramen from the various borders of the ramus will be helpful in the surgeries of maxillofacial region for accurate localization of mandibular foramen and mandibular canal. In a study, in American white and Negros, Giles7 mentioned that the parameters of mandibular ramus like height, minimum and maximum breadth are very important with classification accuracy of 85%8.The author Kilarkaje9 et al. in his study found mandibular foramen within the distance of 25mm from the anterior border, mandibular notch and third molar tooth and stated that there was bilateral symmetry in all the cases he studied while the author Shalini5found bilateral symmetry within the range of 13 to 20 %. On further review of literature, we found following results- As per A.C. Gabriel14the width of ramus and the position of mandibular foramen are inter-related. When ramus width is more, the mandibular foramen is far from the posterior border and is at higher level than the normal location. The width of ramus found to have different values in male and female mandibles. This difference is accounted for the genetic factors, different forces of muscles of mastication and to the nutrition in different studies.15 B Lalitha19 in her study found that the mean horizontal diameter of mandibular foramen on the right side was 3.54 ± 0.65 mm and on the left side was 3.40 ± 0.82 mm while in our study we found it as 4.26mm on the right side where as 4.29mm on the left side. The embryological basis for the occurrence of accessory mandibular foramen has been explained in literatures. Chávez-Lomeli20 et al. had said that inferior alveolar nerve when arises from the mandibular nerve, initially has three divisions later which get fused and a single nerve is formed (60% of cases) which passes through mandibular foramen. In case of non - fusion of these divisions, the unfused divisions or rami (40% of cases) pass through different foramina which are called as accessory mandibular foramina.5 According to Anand Reddy6, accessory mandibular foramina not necessarily pass sensory nerve elements always sometimes instead of nerves they pass blood vessels only. Therefore, the presence of accessory mandibular foramina is not always associated with difficulty in inferior alveolar nerve block. In the study by Hanihara and Ishida21, it is mentioned that Asian males showed higher prevalence of accessory mandibular foramina. Our study is in agreement with this with the incidence of 42.68%.
CONCLUSION There are variations in the morphometry of mandibular ramus which leads to different location of mandibular foramina. So the knowledge of mandibular foramina and related variations will lead to successful inferior alveolar nerve blocks and less postoperative complications in maxillofacial surgery.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.