 Home
Home|
Table of Content Volume 11 Issue 2 - August 2019
Morphometric investigation of occipital condyles and its relevance in transcondylar approach: An observational study in western Uttar Pradesh region
Rakesh Kumar Agarwal1, Anuj Ram Sharma2*, Vishnu Gupta3
1Associate Professor, Department of Anatomy, Maharishi Markandeshwar Medical College and Hospital, kumar Hatti, Solan Himachal Pradesh, INDIA. 2Assistant Professor, 3Professor and HOD, Department of Anatomy, Muzaffarnagar Medical College and Hospital, Muzaffarnagar, Uttar Pradesh, INDIA. Email: dr.anujlatasharma@gmail.com Abstract Background: The knowledge of the occipital condyles diameter and density, shape of condyle, or its articular facet will help the surgeons to decide the extent of bone that can be removed. Therefore, the present study was conducted to have a proper database regarding the morphometric parameters of occipital condyle. Materials and Methods: The study group includes adult skulls of 50 males and 46 females as determined by visual assessment of non-metrical parameters for sex determination of skull. Only those skulls having full cranial base with intact occipital condyles and foramen magnum for all measurements to be taken were included. Measurements were appropriated from respective intact cranial base with the help of sliding calipers. To allow for instrument error, every assessment was obtained in millimeters (mm) with the accurateness of 0.5 mm. Result: When we compare the dimensions of occipital condyle in male and female There is non-significant difference in diameter of each side occipital condyles of both genders (p>.001) and significant difference in maximum distance between occipital condyles of male and female (p<.001). In male and females there is non-significant difference in maximum width both side condyles.(p>.001).Conclusion: These specifications must be assess into contemplation through dorsal and lateral manner to the cranio-vertebral intersection by orthopaedicians and surgeons. Investigations in future are must be required for further more affirm preliminary outcomes obtain with this research. Key Words: Occipital Condyles, Transcondylar, craniocervical instability
INTRODUCTION Occipital bone can be detailed as it is penetrated by the largest foramen called foramen magnum; it is a distinctive and composite region anatomically inside the middle area of the basal part of the bone. The basilar parts of this bone forms anterior margin of the foramen magnum, the both sided ex-occipitalis forms lateral borders and posterior border is bounded by superior occipital area of the bone.1Bean shaped condylar facets are seen on equally present foramen for articulation by the uppermost 1stcervical vertebra at the synovial at lanto-occipital articulation. Individual occipital condyle is the special bony part involving the cranium and the vertebrae. The advancement in neuroimaging techniques has greater interest for aggressive surgery of craniovertebral site, which must be needed the facts related anatomical feature of the craniovertebral connection. Because of its shield anatomical position and deepens of the base of craniam, this portion of the skull tends to unaffected by both physical affront and inhumation somewhat extra advantageous than many other region of the cranium base.2 During the craniovertebral surgery requires alateral approach removal of the condyles. The morphology of the occipital condyles with their facets is clinically very important. Knowledge of Anatomy of the abnormalities of the condyles may be necessary when doing surgical treatment and interpretation of neuro-investigative procedures. Most suitable surgical techniques are to be established for a careful planning mainly based on the morphometric analysis of the foramen magnum and the occipital condyles.3Foramen magnum assessment and the diameter of both occipital condyles are chief components for surgical subjection, as examples with cases of resection of tumour from area along with foramen magnum.4-6 Axial span of the both sided occipital condyles and the anterior intercondylar gap are of a big dimensional significance, particularly at the time of introduction of the vertebral artery or the removal of condyles, as in incident of trans- condylar surgery to show the lesions at the ventro-lateral-clivus and jugular foramen.7-9 The cranium floor is the template on that the face is established and thus finds eminent place in the face reconstruction approch.10 The condylar drilling is an important step in the TCA, and the important question is how much of Occipital Condyle can be removed without damaging nearby structures and causing craniocervical instability.11,12 Hence, the knowledge of the length, width and thickness of the OC, shape of the condyle, and its articular facet will help the surgeons to decide the extent of bone that can be removed. Therefore, the present study was conducted to have a proper database regarding the morphometric parameters of occipital condyle.
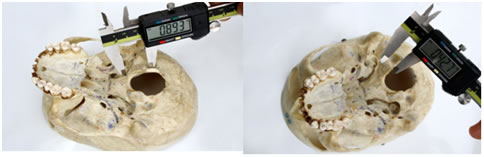
MATERIALS AND METHODS We were collected total 96 human adult skulls from museum of Department of anatomy Muzaffarnagar Medical College, Muzaffarnagar and also from other adjacent medical colleges of same area. The study group includes adult skulls of 50 males and 46 females as determined by visual assessment of non-metrical parameters for sex determination of skull (Krogman’s 1955).13 Only those skulls having full cranial base with intact occipital condyles and foramen magnum for all measurements to be taken were included. Skulls showing any kind of anomalies and skulls with partial damage to foramen magnum area of cranial base were not included. Measurements were assessing from every one intact cranial base with the help of “sliding calipers”. All the measurements were appropriated from respective intact cranial base with the help of sliding calipers. To allow for instrument error, every assessment was noted in millimeters to a precision of 0.5 mm. The subsequent measurements were taken using Holland (1986a):16“Length of both Occipital condyles” –Both occipital condyles length taken by the side by articular surface at right angles to the width of left occipital condyle h (Figure-2).“Maximum width of Occipital condyles” – Both occipital condyles maximum width taken from the articular surface at right angles to the left length of occipital condyle (Figure-3).“Occipital condyle minimum width” – Both occipital condyles minimum width taken from the articular surface at right angles to the length of left side of occipital condyle (Figure-4).“Maximum distance between occipital condyles” - Distance between occipital condyles and its lateral edges at right angles to the midsagittal plane (Figure-5).“Minimum distance between occipital condyles” – Minimum distance between the occipital condyles and its lateral edges perpendicular to the midsagittal plane. “Maximum internal distance of the occipital condyles” –Distance between the occipital condyles medial margin at right angles to the midsagittal plane. Statistical analysis: P <0.001values were accepted as statistically significant. For each measurement, the minimum and maximum diameters were obtained and mean values with standard deviations for both sexes.
RESULTSTable 1: Side differences in the dimensions occipital condyle
Table 2: Gender differences in the dimensions of occipital condyle
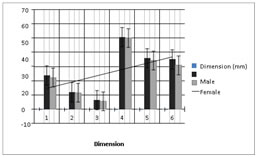
Figure 1: Gender differences in the dimensions of occipital condyle In Males: The value of LOC LENGTH ranged from minimum 23.5mm to maximum 24.1mm with mean value of 23.8 mm and SD of ±0.1. The value of LOC MAX WIDTH ranged from minimum 11.7mm to maximum 12.1mm with mean value of 12.0 mm and SD of ±0.11. The value of ROC LENGTH ranged from minimum 24.5mm to maximum 25.2 mm with mean value of 24.6 mm and SD of± 0.17. ROC MAX WIDTH ranged from minimum 11.9mm to maximum 12.5 mm with mean value of 12.3 mm and SD of ±0.19. In Females The value of LOC LENGTH ranged from minimum 20.2mm to maximum 24.5mm with mean value of 22.3 mm and SD of ±1.06. LOC MAX WIDTH ranged from minimum 10.0mm to maximum 13.3mm with mean value of 11.6 mm and SD of±0.85. Value of ROC LENGTH ranged from minimum 18.5mm to maximum 24.9 mm with mean value of 21.2 mm and SD of ±1.71. ROC MAX WIDTH ranged from minimum 9.5mm to maximum 13.2 mm with mean value of 11.1 mm and SD of ±1.01. Table 1 shows the side differences in the dimensions of occipital condyles and Table 2, figure 1. Shows Gender differences in the dimensions of occipital condyle. Student’s t-test was used to assess if significant differences were present among male and female parameters. The larger space between both Condyles is significantly different for male and females, all other parameters were not significantly different. Figure 2: measurement of Occipital condyle Figure 3: Left occipital condyle maximum width) length with sliding callipers with sliding callipers
Figure 4: Left OC minimum width Figure 5: Maximum distance between OC
When we compare the dimensions of occipital condyle in male and female There is non- significant difference in length of left and Right occipital condyles of male and female (p>.001) and significant difference in maximum distance between occipital condyles of male and female (p<.001). There is non-significant difference in maximum width of right and left occipital condyles of male and female (p>.001). DISCUSSION Comparing the values of different parameters (males) as used in this study and comparing it with Crider’s study (2005) we found that LOC length, Max. span between two condyles, less gap between two condyles and ROC length were smaller in the present study while values of LOC max width, LOC minimum width, Max. Interior distance between condyles, ROC Maximum width, ROC Minimum width and length of basilar process were higher as compared to Crider’s (2005).14 All total diameters were greater in males than females was found by Uysal et al. (2005), with the right condyles measurement lengthwise and the foramen magnum width reflecting the larger dissimilarity same outcome are found in thisresearch.15This is very interesting point pragmatic that all values of female are less than male values, which are shows that these objectives are important for gender identification. These facts are well correlated with the Crider’s study (2005). 14 The huge dissimilarity in among Holland’s (1986a) and the Crider’s are the less Distance among Occipital Condyles and great Interior space between Occipital Condyles.16The occipital condyle is an essential part of the inter section craniovertebral junction. It forms single joint between the occipital and the atlas. Indistinct anatomical feature of these joint outcome in a different biomechanical importance. Its reliability is of essential value for the strength of the cranio vertebral intersection.(Al Mefty et al,1996).17 The role of OC length in occipito-cervical stability has been demonstrated in various biomechanical studies. Removal of same amount of bone stock results in greater occipito cervical instability in shorter condyles compared to longer ones.18,19 This is due to reduction of articular surface area, resulting in hypermobility.18 This hypermobility is normally associated with altanto-occpital joint instability (Caird et al., 2006)20 and can be fatal when accompanied by neurologic complications. Since our study population generally have shorter OC length with females having much shorter condyles, it is conceivable that these groups may be more vulnerable to atlanto-occipital joint instability. The occipital condyles span is essential surgical issue. The outcomes of incomplete condylectomy in a small kind are non-identical from the outcome taken in a long type occipital condyle. Similar number of partial condylectomy may give rise to serious lack of occipito cervical stability in small occipital width. CONCLUSIONThese assessments were done to measure various parameters related to occipital condyle. These specifications must take into contemplation through posterior and lateral approaches to the cranio-vertebral intersection by orthopaedicians and surgeons. Investigations in future are must be required for further more affirm preliminary outcomes obtain with this research. Along with, a relative investigation, with computation from collection of historic and recent skeletal is needed to assess the area of restricted cranial difference that has come.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.