 Home
Home|
Table of Content Volume 11 Issue 2 - August 2019
Anatomical parameters of adult human acetabulum: A cadaveric study
Ilankathir Sridharan1, Sudagar Muthusamy2*, Sridhar Krishnamoorthy3, Sowmiya Ganesan4
1Associate Professor, 2,3,4Assistant Professor, Department of Anatomy, Aarupadai Veedu Medical College and Hospital (Puducherry), Vinayaka Missions Research Foundations, Deemed to be University. Email: anat9799@gmail.com
Abstract Background: There are three bones of the os coxae (hip bone) that come together to form the acetabulum. Contributing a little more than two-fifths of the structure is the ischium, which provides lower and side boundaries to the acetabulum. The ilium forms the upper boundary, providing a little less than two-fifths of the structure of the acetabulum. The rest is formed by the pubis, near the midline. Aim of the study: Reconstruction of the acetabulum in patients with significant acetabular bone deficiency remains a challenge. Hence, the present study was carried out with the aim to study the morphological and morphometric measurement of the acetabulum in the pelvic bone. Materials and Method: 50 cadavers, 25 male and 25 female dry adult hip bones of known gender. A vernier caliper and ruler were used for the measurement. The shapes of the anterior acetabular ridge were noted, and the transverse and superoinferior diameters of the acetabulum were measured using vernier calipers. The data were recorded and analyzed using SPSS. Results: It was observed that the dimensions were greater in males when compared with that of females but the difference was statistically insignificant. On the left side, the parameters measured were greater than those of the right side in both the sexes but of no statistical significance. Conclusion: The knowledge of the anatomical parameters of the acetabulum is of immense importance to the orthopedic surgeons. Hip surgeries are one of the complicated and important procedures which require more detailed knowledge, about the complex acetabular measurements to fulfil the need for verifying the validity of various surgical procedures under practices. Key Words: Acetabulum, Prosthesis, Congenital hip dysplasia, Acetabular diameter, Acetabular depth.
INTRODUCTION The hip joint is one of the major weight-bearing joints of the body. It was originally referred to a ball and socket joint but now it is being described as rotational conchoids 1. The femoral head articulates with a cup-shaped acetabulum, its centre lies a little below the middle third of the inguinal ligament. Movements at this joint include flexion, extension, adduction, and abduction 2. Osteoarthritis of the hip joint is a common condition in western countries and has varied etiology. An incongruous joint is more prone to develop degenerative changes than a joint having normal anatomy. It has been estimated that 25-40% of hip osteoarthritis may be caused by acetabular dysplasia. The dysplastic hip also correlates with the acetabular depth. The normal acetabular depth is 9mm and less than that will lead to conditions like dysplasia 3. The knowledge of normal anatomical features and morphometry of the acetabulum is vital to understand the mechanics of the hip joint. The acetabular images aid the surgeon to determine the correct size of the acetabular cup during total hip arthroplasty and to realign the acetabulum back to normal position 4. A bigger roof of the acetabular cup means a good grip of the head of the femur inside the acetabulum and hence a better result of arthroplasty 5. The main problem for acetabular placement will be positioning the acetabular cup implant and acetabular inclination to the correct location according to its acetabular version and the acetabular depth6. The anthropometric study of the acetabulum may be helpful to the radiologist in diagnosing congenital hip dysplasia, and to the orthopedic surgeons in planning before acetabular surgery, during hip arthroplasty and treatment of hip joint fractures 7.
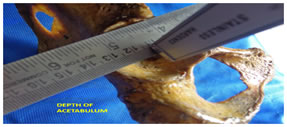
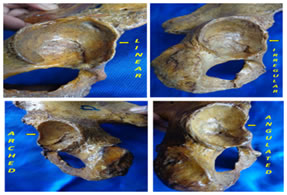
MATERIALS AND METHOD The present study was carried out in the Department of Anatomy, Aarupadai Veedu Medical College and Hospital, Puducherry. The study sample consisted of 50 Human dry hip bones consisting of 25 males and 25 females bilaterally. All the specimens which retained its morphological features and in good condition after dissection from cadaver were used for this study. Specimens with Osteoarthritis of the hip, evidence of trauma or any other skeletal disorders were excluded. Gender classification of the samples was carried out considering the following parameters like the shape of obturator foramen, the width of the greater sciatic notch, muscular markings, ischiopubic rami. Morphological parameters of all the hip bones were observed and tabulated. The shape of the anterior acetabular ridge: varying in shapes of the anterior acetabular ridge were noted and tabulated. Anterior acetabular ridge presented itself with 4 different shapes namely – arched, linear, irregular and angulated. All the Morphological variations obtained were compared bilaterally and between genders. The acetabular diameter (transverse and superoinferior) and depth were measured using a vernier caliper (Mitutoyo, Japan; accuracy: 0.01mm), and the shape of the anterior acetabular ridge was noted. PARAMETERS ANALYSED The transverse diameter of the acetabulum was defined as the maximum distance between the anterior and posterior ends of the acetabular cavity while the superoinferior/ vertical diameter was defined as the maximum distance between the upper and lower margins of the acetabular cavity. The total diameter was defined as the average of the transverse and superoinferior diameter. The depth of the acetabulum was defined as the maximum vertical distance from the deepest point in the acetabular cavity to the brim of the acetabulum. A thin plastic ruler was placed across the diameter of the acetabular cavity and then the depth of the acetabulum was measured on the vernier caliper from the deepest point in the acetabulum to the plastic ruler [Fig.1]. The shape of the anterior acetabular ridge was classified as arched, angular, linear and irregular [Fig.2]. STASTICAL ANALYSIS: The data obtained were tabulated and analyzed statistically to find Mean, Standard deviation (SD) and Range in both the sexes and both the sides. The results were analyzed statistically, by unpaired Students t-test. The p-value of < 0.05 was considered for Statistical significance, Statistical analysis was done using SPSS (Statistical Package for the Social Sciences) version 11 and Microsoft Excel 2007. RESULTS Table 1 Depth Of Ace:tabulum (N = 50; Right = 25, Left = 25)
Table: 1 shows measurements of right side in males were (23.0±34.0) compared with measurements of right side in females (23.0±26.0) (b) measurements of left side in males (27.49±2.70) were compared with left side measurements in females (25.70±2.11) It was observed that the depth of the acetabulum was greater in males than females both on right and left side.
Table : 2 transverse diameter of acetabulum (n = 50; right = 25, left = 25)
Table: 2 shows on the right side the difference being statistically significant (right p=0.02, left P=0.06). It was noticed that the diameter of the left acetabulum was greater than that of the right side in both sexes but the difference was statistically insignificant (male p=0.34, female p=0.20). The diameter of the acetabulum was greater in males than in females Table 3: vertical diameter of acetabulum (n = 50; right = 25, left = 25)
Table: 3 shows There was a significant difference in the vertical diameter of acetabulum between the two sexes (right p=0.04), left p=0.75). In both, the genders left acetabulum had a greater diameter than that of right side but of no statistical significance (male p=0.75, female p=0.06). The vertical diameter of the femoral head was greater in males than in females both on right and left sides. It was also noticed that in both sexes the vertical diameter was more on the left side than the right side though the difference was statistically significant.
Table 4: varying shapes of anterior acetabular ridge
Table: 4 Shows In the present study, the anterior acetabular ridge shapes recorded were compared to those of other researchers. The shape with the highest frequency was the arched shape (30%). The next common shape was the angular shape (25 %,) the linear shape of the anterior acetabular ridge was found to be 25%. It is important to note that the linear and angular shapes had almost the same frequency of occurrence in the present study. The irregular shape has the least incidence amongst all the acetabular ridge shape with a percentage of 20 %.)
DISCUSSION The hip joint is one of the major joints of the body. Though described conventionally as a ball and socket variety of synovial joint, Martin RL et al reports it to be a rotational conchoid. Knowledge of the anatomical parameters of the bony components of the hip joint is very essential as it will open new horizons into a better understanding of the etiopathogenesis of diseases like primary osteoarthrosis of the hip joint.9 An incongruous joint is more prone to develop degenerative changes than a joint having normal anatomy Govsa F, et al Awareness of the average dimensions of the bones of the hip joint in both sexes will also help in early detection of disputed sex by Forensic experts.10 As total hip replacement is a common surgery performed nowadays knowledge of the dimensions of the acetabulum and femoral head will assist, surgeons to construct suitable prosthesis.11 Studying cadaveric hip joints is of immense importance as various dimensions are taken with the soft tissues in place. This gives the average values of various parameters to near normal situations as would be encountered in the patients at the operation table.12 It would be noticed that in the hip joints belonging to males or females, the average diameter of femoral head is smaller than the average diameter of acetabulum impressing upon the fact that the femoral head is snugly fitted into the acetabulum which is one of the major reasons why primary osteoarthrosis of hip joint and is also so uncommon among Indians. Various parameters measured had a higher value on the left side than the right.13 Vix VA et al suggest that left limb is dominant. Whether a person is right-handed or left-handed more people use left lower limb for weight-bearing.14 Siebenrock ka et al Therefore, the dimensions of the bones forming the hip joint of the left side should be more so as to bear greater loading force on the femur. Though, in the present study left hip joint dimensions are greater than the right yet they are statistically insignificant.15
CONCLUSION It was concluded from this study that the regional variations in the parameters measured do exist when the data of two different countries are considered but within a country, there is not much variation. Moreover, in the last four decades, the dimensions of the bony components of the hip joints studied have not changed much. All the diameters and depth of acetabulum were larger in males as compared to females and were found to be statistically highly significant.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.