|
Table of Content Volume 12 Issue 2 - November 2019
Morphology of human liver - A cadaveric study
Abstract Background: Liver is largest gland of body which occupies a substantial portion of upper abdominal cavity. Morphological variations of liver are in form of accessory fissures, shape and number of accessory lobes, etc. Knowledge of these variations and having awareness is useful to the clinicians to rule out the disease, to the radiologist for diagnostic imaging ,for surgeons during segmental resection of liver for favourable surgical outcome. The present study aims to analyse and classify the morphological variations of liver observed during the study. Material and Methods: fifty adult cadaveric human liver preserved in formalin of unknown sex were observed. Different variations in lobes, fissures and accessory lobes, lobar atrophy and any other variations on the surface of the livers were observed. The liver specimens were also classified according to Netter’s six types of morphological liver variations. Results: Out of fifty human cadaveric livers only 4 specimens (8%) were normal in their external appearance and 46(92%) liver specimens showed morphological variations .Out of 46 specimens, accessory fissures were observed in 25 (50%) specimens, pons hepatis joining the left lobe with quadrate lobe was seen in 4(8%) of specimens, Absence of fissure for ligamentum teres was seen in 1 (2%) specimen, elongated left lobe was present in 4(8%) specimens. Mini accessory lobe were seen in 4(8%) specimens. Large papillary process seen in 1 (2%) specimen. According to Netter’s classification, Type 4 (tongue like process of right lobe) seen in 1(2%) specimen. Type 5 (very deep renal impressions and corset constriction) seen in 3(6%) specimen and type 6 (diaphragmatic groove) was seen in 3(6%) specimens. Conclusion: The variations observed in our study will be of great importance to anatomist, surgeons and radiologist.
Key Words: Liver, morphological variations, accessory fissures, accessory lobes, caudate and quadrate lobe, pons hepatis
INTRODUCTION
The liver is wedge shaped, largest gland of the body situated under the right dome of diaphragm and occupies the right hypochondrium and epigastric region. Falciform ligament divides the liver into anatomical right lobe and left lobe, fissure for ligamentum venosum and fissure for ligamentum teres. The additional lobes of liver i.e the caudate and quadrate lobes are parts of right lobe separated from each other by porta hepatis .Inferior surface of liver presents with fossa for gall bladder. Fundus of gall bladder is situated beyond the inferior border1. Morphological variations of liver are in the form of accessory fissures, accessory lobes. Having thorough knowledge of such variations of liver is of great importance to the radiologist for diagnostic imaging, minimal invasive surgical procedures and operating surgeons for favourable surgical outcome2.The present study aims to study the morphological variations of the liver which can be of significance to the anatomist, radiologist and especially surgeons operating to avoid iatrogenic complications during operative procedure.
MATERIAL AND METHODS
The study was conducted in the department of Anatomy of BIMS, Belgaum after obtaining the ethical approval from institutional ethical committee prior to the commencement of the study. Fifty adult cadaveric human livers preserved in formalin of unknown sex were selected for the study. Specimens with pathological findings and damaged liver specimens were excluded from the study. The lobes of liver right lobe, left lobe, caudate lobe and quadrate lobes were studied in detail for their morphological variations and were also classified according to Netter’s classification3 (table no-4) .The specimens were photographed and the observations were noted down.
RESULTS
In the present study, out of fifty (50) human cadaveric livers only 4 specimens (8%) were normal in their external appearance(table no—1/fig no-1). However,46(92%) liver specimens showed morphological variations in form of fissures, lobes, shape and size of lobe, variations were also observed according to Netter’s classification(table no -2,3 and 4 ). As shown in table no- 2, accessory fissures were observed in 10(20%) specimens (fig no -2) on different parts of right and left lobes resulting in accessory lobes. Transverse fissures on quadrate lobe dividing into superior and inferior lobe was observed in 11(22%) specimens (fig no -3). Accessory fissure on caudate lobe dividing it into superior and inferior lobe was seen in 4(8%) specimens (fig no-4). As shown in table no -3, pons hepatis joining the left lobe with quadrate lobe was seen in 4(8%) of specimens( fig no 5).Absence of fissure for ligamentum teres was seen in 1 (2%)specimen ( fig no -6).Elongated left lobe was present in 4(8%) specimens( fig no -7). Mini accessory lobe were seen in 4(8%) specimen(fig no- 8,9) .Large papillary process seen in 1 (2%)specimen( fig no- 10). According to Netter’s classification [table no-4],Type 4 (tongue like process of right lobe ) seen in 1(2%)specimen( fig no-11) .Type 5 ( very deep renal impressions and corset constriction) seen in 3(6%) specimen and type 6 (diaphragmatic groove ) was seen in 3 (6%)specimens ( fig no-12,13). Type 1, 2 and type 3 were not found in any specimens.
Table 1: showing observations in the present study
Observations |
Number of specimens |
Normal specimens |
04 (08%) |
Specimens showing morphological variations |
46 (92%) |
Total |
50 |
Table 2: showing the occurrence of accessory fissures in liver specimens ( n=25)
Observations |
Number of specimens (%) |
Accessory fissures on other lobes |
10(20%) |
Accessory fissures on caudate lobe |
04(8%) |
Accessory fissure on quadrate lobe |
11(22%) |
Liver specimens not showing any fissures |
25 |
Table 3: showing the morphological variations on lobes of liver ( n=14)
Morphological variation |
Number of specimen (%) |
Pons hepatis connecting left lobe with quadrate lobe |
04 |
Elongated left lobe present |
04 |
Mini accessory lobe present |
04 |
Large papillary process and long caudate process |
01 |
Absence of fissure for ligamentum teres |
01 |
Table 4: showing morphological variations according to Netter’s classification(3)(n=7)
observations |
Number of specimens(%) |
Netter type 1( very small left lobe , deep costal impression) |
-- |
Netter type 2 ( complete atrophy of left lobe) |
-- |
Netter type 3 ( transverse saddle like liver ,relatively large left lobe) |
-- |
Netter type 4 ( tongue like process of right lobe) |
01(2%) |
Netter type 5 ( very deep renal impressions and corset constriction) |
03(6%) |
Netter type 6( diaphragmatic grooves) |
03(6%) |
Liver not presenting morphological variations according to Netter’s classification |
43 |
Table 5: Comparison of observations with similar studies
Morphological features |
Joshi SD et al.,[16]
( n=90) |
Muktyaz H and Nema U[2]
(n=41) |
Patil S et al .,[14]
(n=50) |
Nayak BS[17]
(n=55) |
Chaudhari et al.,[18]
(n=80) |
Present study
(n=50) |
Accessory fissures |
30% |
12.1% |
10% |
1.81% |
12.5% |
20% |
Accessory fissures on caudate lobe |
---- |
---- |
---- |
---- |
03.7% |
04% |
Superior and inferior Quadrate lobe |
20% |
---- |
04% |
---- |
07.5% |
11% |
Pons hepatis connecting left lobe with quadrate lobe |
30% |
---- |
10% |
---- |
01.25% |
08% |
Absence of fissure for ligamentum teres |
---- |
09.7% |
04% |
01.81% |
11.2% |
02% |
Riedel’s lobe present |
---- |
----- |
----- |
---- |
01.25% |
---- |
Elongated left lobe present |
---- |
---- |
---- |
01.81% |
12.5% |
08% |
Mini accessory lobe present |
---- |
---- |
02% |
---- |
03.7% |
08% |
Large papillary process |
32% |
---- |
---- |
01.81% |
01.25% |
02% |
 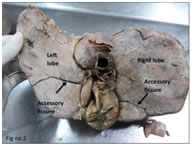 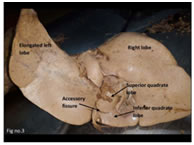
Figure 1 Figure 2 Figure 3
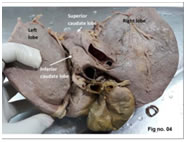 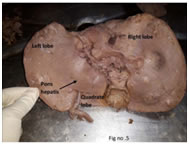 
Figure 4 Figure 5 Figure 6
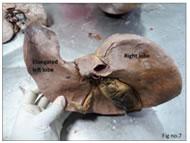 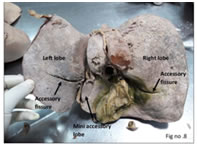 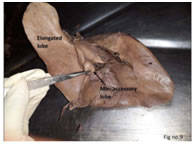
Figure 7 Figure 8 Figure 9
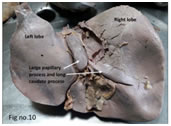  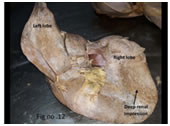 
Figure 10 Figure 11 Figure 12 Figure 13
Figure 1: showing normal morphological features of liver; Figure 2: showing accessory fissures on left and right lobes of liver; Figure 3: showing accessory fissure with superior and inferior quadrate lobe; Figure 4: showing accessory fissure with superior and inferior caudate lobe; Figure 5: showing pons hepatis connecting left lobe with quadrate lobe; Figure 6: showing absence of fissure for ligamentum teres; Figure.7: showing elongated left lobe of liver; Figure 8: showing mini accessory lobe and accessory fissures on right and left lobes; Figure 9: showing mini accessory lobe and elongated left lobe; Figure 10: showing large papillary process and long caudate process; Figure 11: Netter’s type -4 showing tongue like process on right lobe; Figure 12: Netter’s type 5 showing very deep renal impression and corset constriction; Figure 13: Netter’s type -6 showing deep diaphragmatic grooves.
DISCUSSION
The embryological development of liver begins at fourth week of intrauterine life as an ventral out pouch on endodermal tube at the junction of foregut and midgut. The hepatic bud thus formed grows within the ventral mesogastrium, and reaches the septum transversum dividing into right and left branches. Each branch gives rise to cluster of cells, the hepatic cylinders, which eventually form two solid masses. These solid masses are symmetrical and represent the rudimentary right and left lobes of liver. Liver is the most massive of the viscera, occupying the substantial portion of abdominal cavity4. The morphological variations can be congenital malformations of the liver which include agenesis of the lobes, absence of segments, deformed lobes, atrophy of segments and hypoplastic lobes. These anomalies can be due to excessive development or defective development. Sometimes these anomalies can be associated with malformations of other organs like diaphragm and suspensory apparatus of liver5. The lobar and segmental anomalies are rarest of all malformations. The embryological basis of the anomalies of liver morphology occurring in the course of organogenesis remains to be elucidated6.Some of the morphological changes detected during advanced imaging examination may actually be pseudo—lesions resulting from perfusion defects, focal fatty infiltrations and other causes may not represent true parenchymatous lesions7. As shown in table no.1, in the present study 4 specimens showed normal external morphology and 46 liver specimens presented with morphological variations. Comparison of the observations reported by various authors with the present study has been tabulated in table no-5. Accessory hepatic fissures are considered to be the potential source of diagnostic error during imaging , as accessory fissure is the most common morphological variation. In the present study, accessory fissures were observed in 10 specimens on right and left lobes of liver (fig no- 2). Transverse fissure was observed on quadrate lobe dividing it into superior and inferior lobe in 4 specimens and on caudate lobe dividing it into superior and inferior lobe in 4 specimens (fig no- 3,4). The fissures are formed by the invagination of muscular diaphragm into the liver on costal surface .Multiple accessory fissures may mimic pathologic macronodular liver on CT. Fluid collection in these fissures may be mistaken for a liver cyst, liver abscess or implantation of disseminated tumor cells. Hence screening the presence of accessory fissures becomes important during radiological intervention and surgical procedures8. An accessory lobe of liver is an anatomical abnormality that is rarely seen and is mostly due to embryonic heteroplasia. Accessory lobes can be of two types ,an accessory lobe joined to normal hepatic tissue and lobe that is completely separate .It can be classified as pedunculated or sessile9,10.Embryologically accessory lobes are formed by the displacement of the primitive rudiment of the organ or by the persistence of the mesodermal septa during proliferation , which occurs due to defective formation of the caudal foregut and hepatic bud in the third month of the intrauterine life11.Riedel’s lobe is the most commonly occurring variation of the reported accessory lobes12, however Riedel’s lobe was not observed in the present study. Jurkovikj reported small accessory lobe connecting the tuber omentale by mesentry containing portal and biliary elements13.In the present study accessory lobe were present in 4 specimens out of which 3 specimens showed accessory lobe between quadrate lobe and porta hepatis joined to normal hepatic tissue, in another specimen a mass of hepatic tissue projected between the caudate lobe and quadrate lobe of liver(fig no- 8,9). Complications of accessory liver lobe is torsion, especially in pedunculated form which requires emergency surgical intervention14.Mini accessory lobes can be mistaken for lymph nodes and can be removed accidentally during surgery which would result in excessive bleeding in abdomen due to damage to liver lobe or vascular pedicle11.Another morphological variation observed was the presence of pons hepatis. In case of pons hepatis, bridging the fissure for ligamentum teres, normal visualization of the fissure would not be possible and dimensions of the right and left lobes may be mistaken15.Joshi et al, studied 90 liver specimens out of which 30% of liver specimens had variable pons hepatis16 . In the present study, pons hepatis was observed in 4(8%) of specimen( fig no-5), observations are in accordance with Patil S et al., who observed similar findings in 10% specimens out of 50 liver specimens14.Absence of fissure for ligamentum teres was observed in 1(2%) specimen (fig no- 6),similar finding was reported by Muktyaz H and Nema U2. Findings in the present study correlates with BS Nayak17 who also encountered the similar finding in 1.81% of specimen whereas contradicts with the findings of Chaudhari et al who reported the absence of fissure for ligamentum teres in 11.2% of specimens18.Morphological variations of left lobe include hypertrophy of left lobe, hypoplasia of left lobe and presence of fissures15.Atrophy or hypoplasia of left lobe has been reported19.On the contrary, in the present study, Netter’s type 1 and type 2 presentation i.e small or complete atrophy of left lobe was not observed .Instead , elongated left lobe was observed in 4 specimens( fig no- 7,9). Similar observations were reported by Arya R S et al and Nayak BS in 15% liver specimens with tongue like elongation of left lobe and 1.81% livers were reported with extremely long left lobe respectively20,17.Defective development of left hepatic lobe can lead to gastric volvulus ,whereas defective development of right lobe of liver either remains clinically latent or leads to portal hypertension6.The caudate lobe is considered as an independent segment according to Couin and classification .Isolated resection of caudate lobe and resection of caudate lobe combined with major hepatectomy procedures for hepatocellular carcinoma or hilar bile duct carcinoma has increased in number21.Therefore the knowledge of morphological variations of caudate lobe is essential for surgeons. Phad et al., reported enlarged caudate process in 10% of specimens and enlarged papillary process in 5% of specimens15. In an extensive study by Joshi et al., on variations of liver , notching along the inferior border of caudate lobe was found in 18% of liver, a vertical fissure in 30% and prominent papillary process in 32% of specimens16.In the present study , prominent papillary process and long caudate process was observed only in one specimen ( fig no- 10) which correlates with similar findings reported by Nayak BS and Chaudhari et al.,17,18.It was suggested that normal sized or small papillary process on computed tomography may be mistaken for enlarged porta hepatis nodes and when enlarged papillary process extends to left side it can mimic pancreatic body mass22.Acquired changes in the liver morphology are represented by the following characteristic features:1) linguiform lobes 2) costal organ with very small left lobe 3) deep renal impression and corset type constriction and local infiltration of organ of gall bladder23.In the present study , Netter’s type 1,2,3 were not observed among 50 liver specimens ,whereas Netter’s type 4,5 and 6 were observed i.e tongue like process of right lobe was seen in 1(2%) specimen, very deep renal impression and corset type constriction seen in 3( 6%) specimen and diaphragmatic sulci were observed in 3 (6%) specimens( fig no -11,12,13). Diaphragmatic sulci are formed due to irregular growth of liver parenchyma which is caused due to the resistance by different bundles of diaphragm. Diaphragmatic sulci could be a good landmark for projection of the portal fissures and of the hepatic veins with their tributaries running through them24.
CONCLUSION
The findings in this study will help anatomist, radiologist, surgeons to understand the morphological variations of liver which will be helpful for operating surgeons and radiologist to prevent complications and misdiagnosis.
REFERENCES
- Standring S. Gray’s Anatomy: The anatomical basis of clinical practice 40th ed. New York: Churchill Livingstone 2008; 3441-46.
- Muktyaz H, Nema U. Morphological variations of liver lobes and its clinical significance in north Indian population. GJMMS.2013;1(1):1-5.
- Netter FH. Atlas of Human Anatomy. 2ed. New York: 18 Guilford Press, 2000.
- Sultana S, Chandrupatla M, Swargam N, Jyothi A.Elongation of left lobe of liver: A case report. Int. J.of Allied Med. Sci. and Clin. Research 2015;3(2):152-156.
- Daver GB, Bakhshi GD, Patil A, Ellur S, Jain M, DaverNG. Bifid liver in a patient with diaphragmatic hernia.Indian Journal of Gastroenterology2005;24(1):27-28
- Champetier J, Yver R, Létoublon C, Vigneau B. A generalreview of anomalies of hepatic morphologyand their clinical implications. AnatomiaClinica1985;7(4):285-299
- Meirelles GSP, G. D’Ippolito. Liver pseudo lesions in helical CT: pictorial essay. Radiol Bras. 2003;36:229-35.
- Auh YH, Lim JH, Kim KW. Loculated fluid collections in hepatic fissures and recesses: CT appearance and potential pitfaJls. Radiographics. 1994;14:529-40.
- Stattaus J, Kühl H, Forsting MZ. Diagnosis of an accessoryliver lobe established by magnetic resonance imaging-guided core biopsy. Gastroenterol.2008;46(4):351-4.
- Wang C, Cheng L, Zhang Z, Xie T, Ding H, Deng Q et al.Accessory lobes of the liver: A report of 3 cases and review of the literature. Intractable Rare Dis Res.2012 May;1(2):86-91.
- Carrabetta S, Piombo A, Podesta’ R, Auriati L. Torsion and infarction of accessory liver lobe in young man. Surgery. 2009;145:448-49.
- M. Massaro, M.P. Valencia, M. Guzman, J. Mejia, Accessory hepatic lobe mimicking an intra abdominal tumor, J. Comput. Assist. Tomogr. 31 (2007) 572–573.
- D. Jurkovikj, New variant liver surface morphology according to portal vein segmentation, IJAPSA 2 (2016) ISSN :2394–2823X.
- Patil S, Sethi M, Kakar S. Morphological study of human liver and its surgical importance. Int J Anat Res. 2014;2(2):310-14
- V.V. Phad, S.A. Syed, R.A. Joshi, Morphological variations of liver, Int. J. Health Sci. Res. 4 (2014) 119–124.
- SD, Joshi SS, Athavale SA. Some interesting observations on the surface features of the liver and their clinical implications, Singapore Med J.2009;50(7):715-19.
- Nayak BS. A Study on the Anomalies of Liver in the South Indian Cadavers. Int. J. Morphol.2013;31(2):658-661
- Chauhdari H, Ravat M, Vaniya V, Bhedi A. Morphological Study of Human Liver and Its Surgical Importance. Journal of Clinical and Diagnostic Research.2017Jun;11(6): AC 09-AC12.
- S. Vinnakota, N. Jayasree, A new insight into the morphology of the human liver: a cadaveric study, Int. Sch. Res. Notices. 2013 (2013) 689564.
- Arya RS, Arya RC, Kumar A, Basan K, Singh B, Jangde S. Study of Cadaveric Liver Lobe Anomaly. Indian Journal of Clinical Anatomy and Physiology2015;2(4):212-215
- K. Kogure, H. Kuwano, N. Fujimaki, M. Makuuchi, Relation among portal segmentation, proper hepatic vein, and external notch of the caudate lobe in the human liver, Ann. Surg. 231 (2000) 223–228.
- Y.H. Auh, W.A. Rubenstein, K. Zirinsky, J.B. Kneeland, J.C. Parde, L.A. Engel, J.P. Whalen, E. Kazam, Accessory fissures of the liver: CT and sonographic appearance, Am. J. Roentgenol. 143 (1984) 565–572.
- M. F. Royer, Vias Biliares e Pˆancreas, Guanabara Koogan, Rio de Janeiro, Brazil, 1959.
- Macchi V, Feltrin G, Parenti A, De Caro R. Diaphragmatic sulci and portal fissures. J Anat. 2003;202(3):303-08.
|
|
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.