 Home
Home
|
Table of Content Volume 13 Issue 1 - January 2020
Arterial variation in the brachial artery and its clinical implications
Balakrishnan R1, Kavya2*, Sharmada KL3
1Assistant Professor, Department of Anatomy, SRM Medical College Hospital And Research Centre. 2Assistant Professor, 3Tutor, Department of Anatomy, Bowring and Lady Curzon Medical College and Research Institute, Bangalore Email: kavs_084@yahoo.co.in
Abstract Background: Recent progress in vascular surgery has engendered a need for precise knowledge and frequency of anatomical variations in the branching pattern of brachial artery and appreciation of these variations in the upper extremity vasculature is essential to prevent injury, particularly in patients requiring dialysis or undergoing arteriography. Abnormal branching pattern in the vasculature of the upper limb is attributed to the embryonic development of the vascular plexus of the upper limb bud. Aim: Brachial artery being one of the important arteries from clinical point of view, the branching pattern of brachial artery is important in treating cases of arterio-venous fistulae, aneurysms and abscess drainage in the region of axilla, arm and cubital fossa. Particular attention has to be given to the anatomical position of brachial artery while performing cardiac catheterization, intra-arterial injections and angiographic procedures via brachial artery. Considering all these factors, study of vascular pattern of upper limb and its variations assume great importance to prevent and avoid possible complications and achieve best results after surgeries as well as diagnostic and therapeutic interventions Materials and Method: The present study consisted of 78 upper limb specimens of unknown age and sex, for a period of 3 years. The cause of death and past history was unknown. The skin and deep fascia of the upper limb were completely dissected and neurovascular bundle of the arm, forearm and the palm were clearly exposed, the course of the arteries and their branches were thoroughly traced, noted and recorded using a digital camera. Results: 1.Brachial Artery divided into Ulnar and Radial at a higher level than normal in 12 specimens (15.38%). 2. Brachial Artery divided into Ulnar and Radial at a lower level than normal in 6 specimens (7.96%). In one of the specimen’s Brachial artery continues as the deep brachial artery in the cubital fossa and terminate as radial and ulnar artery just proximal to the bicepital tendon (radial and common interosseous) 3.Superficial ulnar artery arises from the anterior aspect of brachial artery 2 cms distal to the lower border of teres major muscle and passed through the flexor retinaculum and entered the palm forming the superficial palmar arch which was incomplete in 1.28% Conclusions: Genetic influences are deemed to be prevalent causes of arterial variation, although other factors like foetal position in utero, first limb movement or unusual muscular development cannot be completely excluded. Vascular anomalies occurring in common surgical sites tend to increase the likelihood of damage during surgery owing to the unusual origin and branching pattern of brachial artery in the present study, hence a sound knowledge of the possible variations in the branching pattern could avoid unnecessary complications. Key Word: brachial artery.
INTRODUCTION Differences in Arterial channels in upper limb are a rule rather than a variation. Although sporadic accounts of arterial anomalies of the upper extremity have been reported since the 17th century, systematic description did not occur until Quain’s review of the literature and analysis of cadaver dissections and angiographic studies. Four main groups of anomalies exist: (1) failure of the primitive artery to recede, (2) failure of the primitive artery to form, (3) aberrant origin of the native vessel, and (4) ectopic location of an otherwise normal vessel. 1.These variations have drawn attention of surgeons, physicians, radiologists and interventionists, because based on anatomical study, new diagnostic and therapeutic approaches can be proposed. The origin of anomalies in the branching pattern of the upper limb arteries is attributed to defects in the embryonic development of the vascular plexus of the upper limb buds. Attention has to be given to the branching pattern of brachial artery while treating the cases of arterio-venous fistulae, aneurysms and abscess drainage in the region of axilla, arm and cubital fossa. Particular attention has to be given to the anatomical position of brachial artery while performing cardiac catheterization, intra-arterial injections and angiographic procedures via brachial artery. Considering all these factors, study of vascular pattern of upper limb and its variations assume great importance to prevent and avoid possible complications and achieve best results after surgeries as well as diagnostic and therapeutic interventions 2. Anatomical variations in the upper limb are frequent, but the coexistence of multiple muscular and vascular variations is rare such variations are noteworthy for clinicians since they influence and interfere in surgical and diagnostic procedures. Brachial artery is the principal artery of the upper limb and begins as a continuation of the axillary, begins at the distal border of the tendon of teres major and ends about a centimetre distal to the elbow joint (at the level of the neck of the radius). In the arm brachial artery gives out profunda brachii, nutrient, superior, middle and inferior ulnar collateral, deltoid, muscular, radial and ulnar arteries and terminates by dividing into radial and ulnar arteries 3.The profunda brachii is a large branch from the posteromedial aspect of the brachial artery, distal to teres major. It follows the radial nerve closely, at first posteriorly between the long and medial heads of triceps, then in the spiral groove covered by the lateral head of triceps. It supplies muscular branches, the nutrient artery of the humerus, and finally divides into terminal radial and middle collateral branches 3.The radial artery arises 1 cm distal to the flexion crease of the elbow. It descends along the lateral side of the forearm giving a radial recurrent branch, cutaneous branches and few muscular branches to the muscles of the radial side of the forearm. At the wrist the radial artery passes on to the dorsal aspect of the carpus between the lateral carpal ligament and the tendons of abductor pollicis longus and extensor pollicis brevis. In the hand the radial artery passes through the first interosseous space between the heads of the first dorsal interosseous and crosses the palm. At the fifth metacarpal base it anastomoses with the deep branch of the ulnar artery, completing the deep palmar arch 3.The ulnar artery arises 1 cm distal to the flexion crease of the elbow and reaches the medial side of the forearm midway between elbow and wrist. Ulnar artery gives anterior and posterior ulnar recurrent arteries, Common interosseous artery, Anterior interosseous artery, Posterior interosseous artery, Posterior interosseous recurrent artery, Cutaneous and Muscular branches in the forearm and then crosses the flexor retinaculum lateral to the uln ar nerve and pisiform bone to enter the palm to form the superficial palmar arch 3.
MATERIALS AND METHODS The present study consisted of 78 upper limb specimens of unknown age and sex, for a period of 3 years. The cause of death and past history was unknown. The skin and deep fascia of the upper limb were completely dissected and neurovascular bundle of the arm, forearm and the palm were clearly exposed, the course of the arteries and their branches were thoroughly traced, noted and recorded using a digital camera.
OBSERVATION
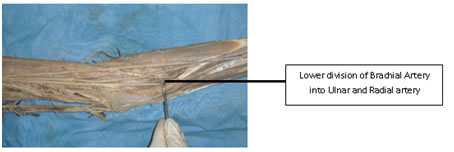
Figure 1:
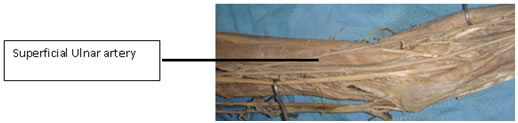
Figure 2: DISCUSSION DISCUSSION The present paper describes the arterial variation in the upper limb. The incidence of anatomical variations of upper limb arteries varies between 11-24% in normal population 4. In a case by reported Chandrika Tali et al profunda brachii artery arose from a common trunk along with superior ulnar collateral artery, posterior circumflex artery in a proximal part of brachial artery before its termination 5. Origin of profunda brachii artery is variable arising as a common trunk with superior ulnar collateral artery amounts to 22.3% and the origin of this artery from posterior circumflex humeral associated with high division of brachial artery has also been reported 5. Ulnar artery is the largest terminal branch of the brachial artery along with the radial artery it supplies the flexor compartment of forearm and palm. Superficial ulnar artery is a rare variation arising from the ulnar artery. It usually arises higher up, either in the axilla or the arm, and runs a superficial course in the forearm before entering the hand 6.The anatomical knowledge of the anomalous branching pattern of the brachial artery is important during percutaneous arterial catheterization, so as to prevent any complications arising from accidental damage to the anomalous vessel 4.In the present study Brachial artery divided at a higher level than usual in 15.34% and lower division was seen in 7. 96% of specimens, in one specimen the Superficial ulnar artery arises from the anterior aspect of brachial artery 2 cms distal to the lower border of teres major muscle and the superficial ulnar artery passed through the flexor retinaculum and entered the palm forming the superficial palmar arch which was incomplete. In a similar study by Vatsala et al2 and a case report by Teli et al 5 a higher origin of the branches of Brachial artery was seen in 16.6% in the earlier. In the present study superficial ulnar artery arose from the brachial artery at the lower border of teres major muscle and passed superficial and lateral to the median nerve and was present superficial to the bicipital aponeurosis, the artery descended obliquely downwards and medially lying superficially over the superficial muscles of the flexor compartment lying between flexor carpi radialis and Palmaris longus passing deep to through the Palmaris longus and flexor retinaculum and giving rise to incomplete superficial palmar arch from which 4 palmar digital branches arose. After the origin of superficial ulnar artery axillary artery continued as brachial artery which was divided into radial and common interosseous artery at the neck of the radius. The incidence of presence of superficial ulnar artery varies between 0.67% and 9.38%, as reported in various studies conducted throughout the world 7. Superficial ulnar artery arises commonly from the brachial artery and less commonly from the axillary artery and amounts to 0.17% to 2% 6, 7, in another study by Vatsala et al 2 Superficial ulnar artery arose from the upper one third of Brachial Artery, in a variation reported by Shankar et al 6 were the Superficial ulnar artery arose from the 3rd part of the Axillary artery. Presence of any arterial variation can complicate any minor procedures lead to grave consequences. Presence of superficial ulnar artery can complicate a minor procedure such as intravenous cannulation. Any arterial variation in cadaveric anatomy is giving more than necessary importance by surgeons and plastic surgeons for their use in reconstructive flap surgeries 8.
CONCLUSION Variations in the origin and course of the principal arteries of the upper limb have been well documented. Genetic influences are deemed to be prevalent causes of arterial variation, although other factors like foetal position in utero, first limb movement or unusual muscular development cannot be completely excluded. Vascular anomalies occurring in common surgical sites tend to increase the likelihood of damage during surgery. Owing to unusual course of superficial ulnar artery, it would be particularly vulnerable to different surgical procedures. Thus, it is important for surgeons and radiologists to be aware of the possible arterial and muscular variations in order to prevent complications during surgical and diagnostic procedure 9.
REFERENCES Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Anatomy (Print ISSN: 2550-7621) (Online ISSN: 2636-4557) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.