 Home
Home
|
Table of Content Volume 13 Issue 1 - January 2020
Spectrum of thoracic vertebral synostosis with its clinical implications and embryological significance
Meera Jacob1, Bindhu Nair2*, Ramakrishna Avadhani3
1Assistant Professor, 2Associate Professor, 3Professor & HOD, Department of Anatomy, Yenepoya Medical College, Mangalore Karnataka. Email: meera_jacob83@yahoo.co.in , rkavadhani@rediffmail.com , nairbindhu@yahoo.com
Abstract Background: During fourth week of intrauterine life sclerotome part of somites migrate around the notochord and the neural tube and undergo a process of resegmentation. Any defect in resegmentation can lead to vertebral anomalies causing neurological defecits. Materials and Methods: Current study was done on 400 dry specimens of assorted vertebrae collected in the Department of Anatomy, Yenepoya Medical College. Bones were observed for fusion at the level of body, transverse process, lamina and spinous process. Three different specimens of fused vertebrae was found. Two cases were of thoracic vertebral synostosis and one case was of cervicothoracic vertebral synostosis. Discussion: The occurrence of vertebral synostosis can be congenital or acquired due to tuberculosis, Juvenile arthritis and it can also occur due to trauma. Knowledge of occurrence of vertebral synostosis is essential to diagnose varied clinical presentations by thorough physical examinations. Clinical implications and embryological significance of these three specimens is discussed in detail for the treatment to be conducted on a righteous path. Key Word: Sclerotome, Vertebral Synostosis, Vertebral anomalies
INTRODUCTION Vertebral column along with intervertebral disc are the manifestations of metamerism1.The main function of the vertebral column being the support of human body and also acting like a pathway for the spinal cord. Since it is formed due to metamerism, fusion of two or more vertebrae can occur partially or completely. Such fusion can occur in the region of cervical, thoracic and lumbar segments2. Fusion of thoracic vertebrae is rarest among all other types which can be congenital or acquired. Study conducted in Lithuanian population showed that vertebral synostosis in cervical region was 2.6%, 1.6% in thoracic level and 0.5% in lumbar segments3. Fusion of vertebrae can occur secondary to juvenile rheumatoid arthritis, tuberculosis or trauma. Congenital fusion can occur during the time of organogenesis due to failure of segmentation of sclerotomes in conditions like KlippelFiel syndrome or other spinal deformities4. There can be ossification of anterior longitudinal ligament in addition to fusion of vertebrae in cases of Diffuse Idiopathic Skeletal Hyperostosis (DISH) or Ankylosing Spondylosis. Presence of such block vertebrae can result in premature degenerative changes due to biomechanical stress in adjacent segments5.Presence of block vertebrae can result in clinical signs like congenital scoliosis with shortening of trunk and scoliosis or lordosis in older children6. So awareness of vertebral anomalies are of great interest clinically because such abnormalities can result in pain ,muscular weakness and sensory deficits and also compression of neural structures and cerebrospinal fluid channels5.7. So the current study was undertaken to know the site of vertebral fusion ,extent of fusion. Morphometry of the fused vertebrae were also taken for the precise clinical diagnosis and treatment. METHOD OF STUDY Present study was conducted in the department of Anatomy, Yenepoya Medical College Mangalore. Study was done on 400 dry specimens of adult vertebrae of unknown sex. Any variations from normal anatomy was noted like abnormal fusion of adjacent vertebral bodies, pedicles, laminae, spines or transverse process. Broken, damaged or neonatal vertebrae were excluded from the study. appropriate measurements were taken and tabulated.
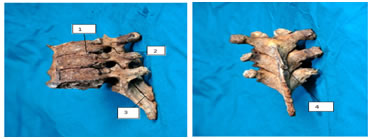
OBSERVATIONS In the present study we found three sets of fused vertebrae among 400 dry specimens of assorted vertebrae. Thoracic vertebral synostosis:- Case1:- In which two thoracic vertebrae were fused as a single functional unit. There was fusion of vertebral bodies in the median plane. The lamina and spines of the vertebrae were also fused. The transverse processes of the vertebrae were separate, and the costal facets seen on either side of the body near its junction. Inferior costal facet of the lower vertebra showed a bony spur which projected downwards (Fig1). Various dimensions of fuse vertebrae is shown in table 1. Case 1: Showing dimensions of one set of fused vertebrae
Figure 1: Left lateral view and posterior view showing fusion between 2 thoracic vertebrae.1.fused body ,2. bony spur,3. Fused facets 4. Fused lamina and spine Case 2:- In this three typical thoracic vertebrae were fused .Bodies of all vertebrae were fused in the anterior median line, articular process were also fused on either side. there was also complete fusion of laminae and spines of all the vertebrae. The spines of lower 2 vertebrae was elongated compared to normal (fig). Various dimensions of fused vertebrae are taken and shown in table no 2. Table 2: showing dimensions of 2 set of fused vertebrae
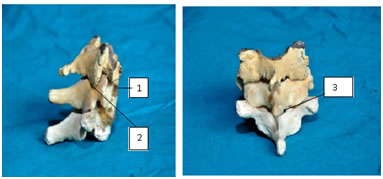
Figure 2: Lateral and posterior view of fusion of three thoracic vertebrae .1.fused body, 2. Fused articular facets 3. Elongated spine, 4. Fused lamina and spinous process Case 3:- was a cervico thoracic synostosis. In this C6, C7 and T1 were fused as a single unit. Vertebral bodies and articular process were fused together. There was fusion of lamina completely on the right side and partially on left side. Spines of all three vertebrae were separate. Figure 3: showing cervico thoracic synostosis.1. Fused body,2. Fused articular facets, 3.Partial fusion of lamina Case 4:- thoracic vertebral synostosis :- in this case 9 thoracic vertebrae were fused .there was fusion of vertebral bodies anteriorly. thelaminae were also fused. spines of middle two vertebrae were elongated and fused with the lower vertebrae. transverse process were separate and costal facets were seen on either side of the body. fusion was seen at the level of costal facets also. Table 4: showing dimensions of fused vertebrae
Embryological development of spinal column is a complex and well regulated process, if disrupted can lead to various congenital anomalies like vertebral synostosis, hemivertebrae etc8.Vertebrae develop from sclerotome part of somites in paraxial mesoderm. Around 4th week it makes its appearance in the cervical region and increases craniocaudally. sclerotome cells then migrate towards the vertebral centrum, neural process and costal process. Ossification centres make their appearance one for the body and one each for neural process9. The development of definitive vertebrae occurs during the time of organogenesis by differentiation and resegmentatation. Inappropriate segmentation can result in vertebral synostosis and spinal fusion. Embryological time of synostosis can be determined when the pedicles and transverse process are not fused showing that initial development was normal10.Clinically vertebral synostosis can lead to various abnormalities like asphyxiating thoracic dystrophy caused by narrow thorax and short ribs11.Apart from this vertebral synostosis can be associated with various complications12 as mentioned below
Pathological causes of block vertebrae are pathological juvenile rheumatoid arthritis, fibrodysplasia, ossification of posterior longitudinal ligament of cervical spine, posttraumatic and postsurgical13. It can cause changes in postural biomechanics and cause degenerative changes and disc prolapsed as age advances14. Since intervertebral disc forms 1/5th of the vertebral column, absence of the disc can lead to shortening of vertebral column and trunk. Thoracic vertebrae with intervening disc along with ribs help in maintaining the shape and stability of thorax. So fusion of vertebrae can narrow thorax and lead to respiratory distress due to Asphyxiating thoracic dystrophy15, 16 Conclusion:- vertebral synostosis results due to failure of resegmentation of vertebrae during organogenesis. It can be congenital or acquired occurring in the cervical, thoracic and lumbar region with varied clinical presentation. Knowledge of any variation from normal anatomy is important for orthopaedician, neurologists and forensic pathologists for proper diagnosis and treatment.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Anatomy (Print ISSN: 2550-7621) (Online ISSN: 2636-4557) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.