|
Table of Content Volume 13 Issue 1 - January 2020
A study of relation of recurrent muscular branch of median nerve to flexor retinaculum in cadavers
Abstract Background: Recurrent muscular branch supplies the muscles of thenar eminence which are responsible for thumb movement. Its relation with the flexor retinaculum of palm has got surgical significance. Aim: To study the relation of recurrent muscular branch of median nerve to flexor retinaculum. Materials and Methods: The study was done on 36 formalin fixed cadavers (72 upper limbs). Results: Out of 36 formalin fixed cadavers (72 upper limbs), 93.05% specimens showed the extraligamentous origin of recurrent muscular branch while 6.95% specimens showed the subligamentous type of origin. Conclusion: Proper understanding of the relation of recurrent muscular branch with flexor retinaculum is helpful in the prediction of the outcome of carpal tunnel surgery.
Key Words: Extraligamentous, Flexor retinaculum, Median nerve, Recurrent muscular branch, Subligamentous
INTRODUCTION
Median nerve gives muscular branch to the thenar muscles in hand called the recurrent muscular branch. The recurrent muscular branch innervates the muscles of thumb i.e. abductor pollicis brevis, opponens pollicis and superficial part of flexor pollicis brevis muscle.1 This branch is of special concern for the surgeons operating on the patient with carpal tunnel syndrome. The branching pattern of recurrent muscular branch has been described with respect to the flexor retinaculum or the transverse carpal ligament (TCL) in various literatures. The transligamentous variant pierces the flexor retinaculum and is considered as the ‘high risk’ variant. The subligamentous variant originates underneath the retinaculum (skandalakis et al) 2 while the extra ligamentous variant arises distal to the flexor retinaculum.
MATERIALS AND METHODS
The study was conducted on upper limbs of 36 formalin embalmed cadavers in a tertiary care hospital of Maharashtra. Due permission was obtained from the ethics committee of the institution. The upper limb specimens were dissected conventionally following Cunningham’s practical manual and the relation of origin of recurrent muscular branch (RMB) of median nerve with respect to flexor retinaculum was observed in palm region. Descriptive statistical method was used for analysing the data.
OBSERVATIONS AND RESULT
The mean distance of origin of recurrent muscular branch from the proximal border of flexor retinaculum was measured to be 21.74±6.67mm. Out of the total 72 specimens, 67 specimens showed extraligamentous origin of the nerve while remaining 5 specimens showed subligamentous origin of the nerve.
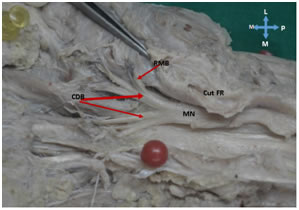
Figure 1: Illustrations showing branch of median nerve in palm; FR: Flexor retinaculum; RMB: Recurrent muscular branch; CDB: Common digital branch; MN: Median nerve P: Proximal D: Distal; M: Medial; L: Lateral
DISCUSSION
Lots of studies which were conducted on recurrent muscular branch of median nerve had referred the Poisel3 classification system. Poisel distinguished three types of branching: the extraligamentous (type I), the subligamentous (type II), and the transligamentous (type III). In the extraligamentous type, which Poisel reported to be the most common, the branch arose distal to the flexor retinaculum and then took a retrograde course to reach the thenar muscles. In subligamentous type, branch arose within the carpal tunnel while in transligamentous type, the branch arose within the carpal tunnel and then pierced the retinaculum. Transligamentous branch is supposed to be at a higher risk of getting damaged during carpal tunnel surgery. Lanz4 had classified these variations into four groups. I-variation in the course of the thenar branch; II-accessory branches at the distal portion of the carpal tunnel; Ill-high divisions of the median nerve; and IV-accessory branches proximal to the carpal canal. Present study results are comparable with the study done by Kozin5 et al. in Philadelphia in 1998.
Study |
Year |
Country |
Specimens |
Results (%) |
Kozin et al.5 |
1998 |
Philadelphia, USA |
202 |
93 EL
7 TL |
Senanayake et al.6 |
2009 |
Sri Lanka |
60 |
88 EL
12 SL |
Bindurani et al.7 |
2011 |
India |
50 |
88 EL
12 TL |
Mizia et al.8 |
2012 |
Poland |
60 |
78.3 EL 20 SL
1.7 TL |
Present study |
(2018) |
India |
72 |
93.05 EL
6.94 SL |
CONCLUSION
The variations in the pattern of recurrent muscular branch is not uncommon and the documentation of these variations are useful for the carpal tunnel release surgery both open an endoscopic.
REFERENCES
- Standring S, Ellis H, Healy JC, Johnson D, Williams A, Collins P, et al. Forearm and Hand. In: Gray’s Anatomy – The anatomical basis of clinical practice. 41th ed. Edinburgh: Churchill Livingstone; 2016: pp. 858-891
- Skandalakis, J. E.; Colborn, G. L.; Skandalakis, P. N.; McCollam, S. M. and Skandalakis, L. J. The carpal tunnel syndrome. Part III. Am. Surg., 58(3):158-66, 1992.
- Poisel S. Ursprung und Verlauf des R. muscularis des Nervus digitalis palmaris communis I (N. medianus), Chir Praxis 18: 471–474, 1974.
- Lanz, U. Anatomical variations of the median nerve in the carpal tunnel. J. Hand surg. 2:44-53, 1977.
- Kozin SH. The anatomy of the recurrent branch of the median nerve. Journal of Hand Surgery. 1998 Sep 1; 23(5):852-8.
- Senanayake KJ, Salgado S, Fernando R. Course pattern of the muscular branch of the median nerve in Sri Lankans hand.
- Bindurani MK. Lokesh HM. Study of Muscular branches of median nerve to the pronator teres. National journal of Clinical Anatomy, 2013; 2(2):67-70.
- Mizia E, Tomaszewski KA, Goncerz G, Kurzydło W, Walocha J. Median nerve thenar motor branch anatomical variations. Folia morphologica. 2012;71(3):183-6.
Policy for Articles with Open Access:
Authors who publish with MedPulse International Journal of Anatomy (Print ISSN: 2550-7621) (Online ISSN: 2636-4557) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal.
Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.