 Home
Home
|
Table of Content Volume 13 Issue 2 - February 2020
Formation of Superficial palmar arch and its clinical relevance - Cadaveric study
Vandana R1*, Ravikumar2
{1,3Assistant Professor, Department of Anatomy} {2Assistant Professor, Department of ENT} Raichur Institute of Medical Sciences Raichur, Karnataka, INDIA. Email: drvandanar@gmail.com
Abstract Background: Superficial palmar arterial arch is a dominant vascular structure of the palm. It is defined as the is an arterial arcade, formed by superficial branch of the ulnar artery and completed on lateral side by the superficial palmar branch of the radial artery or Arteria radialis indicis or Arteria princeps pollicis or arteria nervi mediana. Variations can occur in the vessels contributing to the formation of superficial palmar arch (SPA). Aim: The main objective of the study is to know the formation of superficial palmar arch and different types of formation with an emphasis on its clinical relevance. Result: In the present study was conducted on 30 specimens, we followed classification of Coleman and Anson. We found 75% complete arches and 25% incomplete arches. In complete variety type A and B were equally prevalent. The prevalence of incomplete arches was 25%, most common type of incomplete arch was, Type –B of group II. Some other variations were also found which are mentioned in the article. Conclusion: Knowledge of such variations is of immense help for microvascular surgeons, plastic surgeons and orthopaedicians to bring a better outcome in their surgical procedures. Also it will be helpful for cardiovascular surgeons to carryout radial artery harvesting procedures for the purpose of Coronary Artery Bypass Grafting. Key words: Complete, Incomplete, Coronary Artery, median artery, superficial palmar arch, ulnar artery.
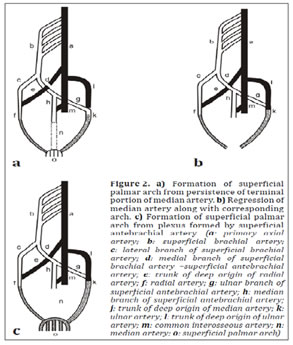
INTRODUCTION The arterial supply of the hand on the volar aspect consists of two systems, superficial and deep palmar arches. The superficial palmar arch (SPA) is arterial arcade that lies superficial to everything in the palmar compartment, i.e. in contact with deep surface of palmar aponeurosis. SPA is formed by the direct continuation of ulnar artery beyond the flexor retinaculum, it is often not a complete arch. If it is complete, it becomes complete with the superficial palmar branch of radial artery. It is completed on radial side either by arteria princeps pollicis, arteria radialis indicis or arteria nervi mediana.1 The arterial system develops from a multiple and a plexiform source, by sequential pattern of development, and functional dominance followed by regression of some path. Developmentally lateral branch of seventh intersegmental artery communicates with axis artery developing in situ in upper limb bud. This axis artery is represented by axillary, brachial, and interosseous arteries. The interosseous artery continues into hand plexus, and forms deep palmar arch. The ulnar, median, and radial arteries sprout from axial artery. Median arteries that sprout from axis artery usually accompany median nerve in hand and forms superficial capillary plexus Median artery regresses, loses its distal connection and superficial palmar plexus is fed by communication of the ulnar artery with the plexus to form the arch.2
Variations in the superficial palmar arch have been studied by several authors. The palm is entirely supplied by both the SPA and deep palmar arch (DPA) with their anastomosis. Vessels of the palm bleed profusely but at the same heal rapidly as like the scalp owing to a good anastomosis. A detailed study of the functions of the hand is the basic requirement of all aspiring hand surgeons. The knowledge of variations of vascular patterns of hand gained more importance in microsurgical techniques, reconstructive hand surgeries, preoperative screening of radial artery harvesting for myocardial revascularization and also in arterial interventions that include radial artery cannulation and radial artery forearm flap. 3 Study is performed in the department of Anatomy at Raichur Institute of Medical Sciences, Raichur, Karnataka. Both right and left palms of twenty formalin- preserved cadavers are dissected. The dissections of hands were performed as per the Cunningham’s manual of practical anatomy.4 The course and branches of the radial and ulnar arteries in the hand were meticulously dissected, the formation of SPA was studied and the variations were observed. Inclusion criteria: Intact palms of disarticulated upper limb specimens. Exclusion criteria: we exclude those palms of hands with some pathologies, previous injury, fractures before death and also fractures after death due to poor handling during transport and storage and any kind of surgeries on hands, as all above conditions may alter the arch pattern and may mislead to our study.
RESULTS In the present study we found 75% complete arches and 25% incomplete arches.
In one complete arch formed by ulnar artery(ulnar type) alone is reaching 1st web space and dividing in two branches and trunk of radial artery in same space dividing into APP and ARI which are anastomosing with each other in this fashion (fig-3). In one specimen with complete classical type of SPA there was a proximal communication between arteries constituting the arch. ARI and APP are arising from as shown in (figure-4). The prevalence of incomplete arches in our study was 25%, seen in 10 specimens. Most common type of incomplete arch was, Type –B of group II, by Coleman and Anson i.e. SPA formed by ulnar artery but does not supply thumb and index fingers, was seen in 5 specimens (12.5%). Next most common type of incomplete arch was type-C of Group II, i.e. SPA formed only ulnar and median arteries but without anastomosis. In one of the incomplete Type –C SPA medial two and half digits are supplied by digital branches of ulnar artery and lateral two and half fingers supplied by digital branches from median artery, it was 50:50 in distribution. And the least prevalent incomplete type was Type-A of Group II, SPA formed by superficial branches of radial and ulnar arteries which was seen only in one specimen. Here APP and ARI were arising from superficial branch of radial artery. Like previous studies on SPA, in present study we also have observed majority of the complete superficial palmar arch and shown in table no-1 Table- no- 1 Results of present study(Classified as per Coleman and Anson Classification)
Table -2: Different types of SPA by various authors along with present study
Figure 1 Figure 2 Figure 3 Figure 4 Figure 1: complete-SPA (Type-B, Ulnar type); Figure 2: complete SPA, Type-C, Mediano-ulnar; Figure-3: showing Type-B with anastomosis in 1st web space; Figure-3: showing Type-B with anastomosis in 1st web space Figure-4: Complete classical SPA Type-A, with proximal communication DISCSUSSION The arterial supply of the hand on the volar aspect consists of two systems, superficial and deep palmar arches. The superficial palmar arch (SPA) is arterial arcade that lies superficial to everything in the palmar compartment. SPA is formed by the direct continuation of ulnar artery beyond the flexor retinaculum, it is often not a complete arch1. Superficial Palmar arch: Owing to a large number of variations in SPA, Poirier (1886) had found it extremely difficult to establish a type, while Adachi (1928) has described 3 types of superficial palmar arch.
Huber (1930) groups the superficial palmar arch into 2 classes:
Group I: Complete arch (Found in 78.5% cases). It can be further divided into five types:- Type A: The classical radio ulnar arch is formed by superficial palmar branch of radial artery and the larger ulnar artery. It was found in 34.5% dissections. Type B: This arch is formed entirely by ulnar artery. It was found in 37% cases. Type C: Mediano ulnar arch is composed of ulnar artery and an enlarged median artery. It was found in 3.8% specimens Type D: Radio-mediano-ulnar arch in which 3 vessels enter into the formation of arch. It was found in only 1.2% dissections. Type E: It consists of a well formed arch initiated by ulnar artery and completed by a large sized vessel derived from deep arch. The latter vessel comes to superficial level at the base of the thenar eminence of join the ulnar artery. It was found in 2% cases. Group II: Incomplete arch: When the contributing arteries to the superficial arch do not anastomose or when the ulnar artery fails to reach the thumb and index finger, the arch is incomplete, such type of arch was found in 21.5% cases. It can be further divided into 4 types. Type A: Both superficial palmar branch of radial artery and ulnar artery take part in supplying palm and fingers but in doing so, fail to anastomose. It was found in 3.2% cases. Type B: Only the ulnar artery forms superficial palmar arch. The arch is incomplete in the sense that the ulnar artery does not take part in the supply of thumb and index finger. It was found in 13.4% dissections. Type C: Superficial vessels receive contributions from both median and ulnar arteries but without anastomosis. It was found in 3.8% specimens. Type D: Radial, median and ulnar artery all give origin to superficial vessels but do not anastomose. It was found in 1.1% cases. 6 The SPA is classified into two categories: complete or incomplete. An arch is considered to be complete if an anastomosis is found between the arteries constituting it. An incomplete arch has an absence of a communication or anastomosis between the arteries constituting the arch. This classification is currently in use and provides the simplest understanding of the anatomic distribution of the arches.7 Coleman et al observed the complete form in 78.5% and incomplete form in 21.5% of 650 hands.8Ikeda et al demonstrated 96.4% complete and 3.6% incomplete forms. 9 The complete SPA was observed in 90% and incomplete SPA was observed in 10 % of cases by Loukas et al10. Complete formation in 78% and incomplete formation 16% in specimens by Patnaik et al 5, complete arch in 84% and incomplete arch in 16% by Al-turk et al.11Complete arch in 72.5% and incomplete arch in 27.5% by Archana et al 2018 12and Chandini Gupta observed 77.3% complete % 22.6% incomplete types.13 Our study shows complete arch in 75% and incomplete arch in 25% of specimens, the values which close to study done by Coleman and Anson ,Chandini Gupta and Archana et al. (table-2) In our study the formation of complete SPA by the linkage or anastomosis between superficial branch of ulnar and radial arteries i.e. the classical type of SPA was found in 35 % of the specimens. Coleman andanson ,Loukas et al , ,Madhystha et al, Suma MP et a and Archana et al observed the classical type of SPA in 34.5%, 40% ,93%, 95% and 35% respectively, the values are very close to Coleman and it is equal to the values observed by author Archana et al. Among the complete SPA formed only by ulnar artery i.e. type B found in 35% of specimens by Loukas, Coleman and anson found in 37% of specimens , Arrchana et al in 27.5%, apart from this many authors have reported case reports of SPA formation by ulnar artery alone like Geethadevi 14, Sharmishta Biswas15, and VR vallola16 respectively. During our study we observed SPA formed by ulnar artery i.e. type- B SPA, in 35 % of specimens, our values are equal to the values of Loukas et al and very close to Coleman and Anson. In one complete arch formed by ulnar artery(Ulnar type) is reaching 1st web space and dividing in two branches and trunk of radial artery in same space dividing into APP andARI which are anastomosing with each other in this fashion (Shown in figure-3) ,such variation is not reported by any authors so far. The median artery (MA) is the axis artery of the superior extremity during early embryonic life. It maintains the superficial palmar arch while the radial and ulnar arteries are developing. The persistence of the median artery in the human adult has been considered as the retention of a primitive arterial pattern. The incidence of median artery is between1.5%-27.1% .The origin of the median artery has been previously described as arising from the ulnar, interosseous, radial,brachial arteries. Association of a persistent median artery with the median nerve should be considered in the evaluation of all patients with carpal tunnel syndrome. kavitha17 . A persistent median artery may take part in SPA in different patterns. Coleman and Anson in their study reported the contribution of median artery to SPA in 9.9 %, among which 3.8 % of specimens were complete mediano ulnar type, 1.2% complete radio mediano ulnar type, 3.8% incomplete mediano ulnar and 1.1% incomplete radio mediano ulnar type .Mamatha Tonse et al observed mediano ulnar type of complete arch in 12% 18. Takkallapalli Anitha et al in their study, found median artery contribution to SPA in 6% of specimens, of which 4% showed complete mediano ulnar type and 2% showed incomplete mediano ulnar type .19 In study by Archana, persistent median artery taking part in SPA was found in 15% specimens, of which 7.5% specimens is of complete mediano ulnar, 2.5% is of complete radio mediano ulnar type and 5% specimens is of incomplete mediano ulnar type. In the present study persistent median artery was seen in 15% of specimens, in which complete mediano-ulnar type was present in 5% and incomplete mediano –ulnar type was observed in 10% of the specimens. Our values are similar to study done by Archana but types of SPA formed by persistent arteries were different.
CONCLUSION The present study has revealed details about some of the variations of superficial palmar arch in humans cadavers which will be supplementing to our already existing knowledge of variations .Variations in the vascular pattern of the hand have been the subject of many studies; these variations may serve as substantial interest to orthopedic surgeons, plastic surgeons, radiologists, and anatomists. These variations are in mode of origin or branching pattern, unexpected relationship with surrounding structures and occupation of unusual tissue planes. In addition, the identification of any variation in the arterial pattern of the hand using Doppler ultrasonography, photo plethysomography and oximetric techniques acquires great importance in various surgical interventions in the hand. Our study gives the necessary information to understand the vascular architecture and its common and rare variations in the hand. REFERENCES
Authors who publish with MedPulse International Journal of Anatomy (Print ISSN: 2550-7621) (Online ISSN: 2636-4557) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.