 Home
Home
|
Table of Content Volume 14 Issue 1 - April 2020
Study of anatomical variations of foramen ovale and pterygoalar bar with it’s clinical significance
Vaishali Sitaram Kirwale¹, Shivaji B Sukre²*
1Assistant Professor, 2Professor & HOD, Department of Anatomy, Government Medical College Aurangabad, Maharashtra, INDIA.
Abstract Background: The foramen ovale is present in the greater wing of the sphenoid bone. The foramen ovale gives passage to mandibular nerve, lesser petrosal nerve, accessory meningeal artery and emissary vein. The present study gives details of variations of foramen ovale and also the incidence of pterygoalar bar in dry human skulls. Materials and Methods: The present study was carried out by using 112 adult dry human skulls. The skulls were examined from the department of Anatomy, Government Medical College Aurangabad. The skulls were carefully observed for the presence of foramen ovale and it’s variations. The length and width of Foramen ovale was measured using digital vernier calliper. Results: The oval shaped foramen was present in 66.07% of skulls. Almond shaped foramen were observed in 14.28% of skulls and round shaped in 10.72% of cases. D shaped foramen was noted in 7.15% cases whereas 1.78% of skulls showed presence of triangular foramen ovale. The mean length of foramen ovale on right side was 7.52+1.15 mm and 7.29+1.06 mm on left side. The mean width of foramen was 4.18+0.78 mm and 4.28+0.81 mm on right and left side respectively. Conclusion: The present study shows wide anatomical variations in foramen ovale. The different shapes like oval, almond, rounded, D shape, triangular were found and abnormal outgrowth like presence of bony pterygoalar bar, spur were also noted in the present study. Key Words: Foramen ovale, human skulls, spur, pterygoalar bar
INTRODUCTION The foramen ovale lie lateral to the Foramen lacerum on infratemporal surface of greater wing of the sphenoid bone. It is present near to the posterior margin of lateral pterygoid plate.1 foramen ovale is located posterior to foramen rotundum, posterior end of carotid groove and just lateral to lingula.2 The foramen ovale transmits the mandibular nerve, lesser petrosal nerve, accessory meningeal branch of maxillary artery and a venous plexus that connects the cavernous sinus to the pterygoid venius plexus in the infratemporal fossa.1,3,4 The mandibular branch of trigeminal nerve passes from the trigeminal ganglion in the cranium through the foramen ovale in the plane of the lateral pterygoid plate. In the foramen ovale it is joined by the entire motor root of the trigeminal nerve and emerges from the skull as a mixed nerve.5 Sphenoid bone ossified by intramembranous and enchondral ossification during 7th month of intrauterine life, the foramen ovale appears as a prominent ring shaped area. The foramen ovale clearly visible 3 year after the birth of the baby.6 The foramen ovale is located at a transition zone between intracranial and extracranial structures.7 It has intense clinical significance in various therapeutic procedures. It gives best neurological information by placing electrodes at foramen ovale during electroencephalography8. Percutaneous biopsy can be done through the foramen ovale in patients with cavernous sinus tumours.9 Study of variations of foramen ovale is very essential in order to treat the patients of trigeminal neuralgia as Gasserion ganglion can be approached transcutaneously through the skull base via foramen ovale.10 The present study provides detailed information regarding variations in shape, size of foramen ovale, morphometric measurements like length and width of foramen ovale and incidence of pterygoalar bar in 112 dried adult human skulls.
MATERIALS AND METHODS In this study 112 was adult dry human skulls of unknown sex were used. The skulls were examined from the department of Anatomy, government medical college Aurangabad during the year 2019-2020. The skulls were carefully observed for the variations of foramen ovale at the greater wing of sphenoid bone by naked eyes. The anteroposterior (length) and transverse (width) diameter of foramen ovale was measured by using digital Vernier calliper. Measurements were taken in millimeters. The obtained data was properly recorded and tabulated. The photographs were taken and findings were compared with previous studies by different authors.
RESULT In the present study 112 dry adult human skulls were used. The shape of the foramen ovale was observed for it’s variations. The oval shaped Foramen was found in majority of skulls, about 148 (66.07%) foramen were oval in shape. Almond shaped foramen was observed in 32 (14.28%) cases. Twenty four, 24 (10.72%) foramen were rounded in shape and 16 (7.15%) were 'D' shaped. Only four (1.78%) skulls showed presence of triangular shaped foramen. All the skulls showed presence of foramen ovale on both sides, none of the skull was with absent foramen ovale. Slit shaped foramen ovale was not observed in any of the skull. Double and confluent foramen ovale was also not found in any skull. (Table no.1) The mean length of foramen ovale on right side was 7.52+1.15 mm and on left side was 7.7.29+1.06 mm. The maximum length of foramen ovale on right and left side was 10.1mm and 9.7mm respectively. The minimum length of foramen ovale on right side was 5.52mm and on left side was 5.43mm. The mean width of foramen ovale was 4.18+0.78 mm on right side and on left side was 4.28+0.81 mm. The maximum width was 6.56mm and 6.30mm on right and left side respectively. The minimum width was 2.87mm on right side and on left side was 2.5mm. Statistical analysis was done by using paired t test to calculate the difference between right and left side. In all parameters (length and width) comparison between two sides was not significant statistically. (Table no.2) In the present study the bony spur in foramen ovale was present unilaterally in 4 cases. None of the skull shows bilateral presence of bony spur. The complete pterygoalar bar was found unilaterally in seven cases whereas one skull shows incomplete presence of unilateral pterygoalar bar. Bilateral complete pterygoalar bar was present in only one skull.(Table no.3) Table 1: Variations of Foramen Ovale with percentage
Table 2: Measurements of foramen ovale In millimeters (mm) with statistical analysis
Table 3: Incidence of pterygoalar bar in the present study
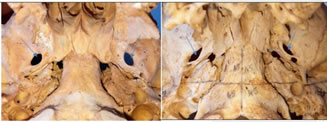 Photo 1 Photo 2 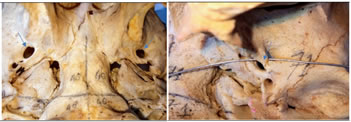 Photo 3 Photo 4  Photo 5 Photo 6 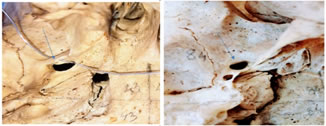 Photo 7 Photo 8  Photo 9 Photo 10 Photo 1: Bilateral oval shaped Foramen ovale; Photo 2: Bilateral almond shaped Foramen ovale; Photo 3: Oval shaped foramen on right and rounded on left side; Photo 4: Presence of Complete pterygoalar bar; Photo 5: Triangular foramen ovale; Photo 6: Foramen ovale with bony spur; Photo 7: Complete pterygoalar bar present; Photo 8: D shape foramen ovale present; Photo 9: Incomplete unilateral pterygoalar bar; Photo 10: small spur in foramen ovale
DISCUSSION The position of foramen ovale is very important in different surgical and diagnostic procedures like compression of Gasserion ganglion in trigeminal neuralgia cases, electroenceplalographic study of temporal lobe in the epileptic patients.11 The reason behind variations in shape of foramen ovale were lies in the developmental process.12 The pterygoalar and pterygospinous ligaments devide the foramen ovale into two compartments, due to these ligaments the transcutaneous needle placement into the foramen ovale become very difficult.13 The surgeon should have knowledge of variations of foramen ovale while performing transovale procedures, as the presence of spur, confluent emissary sphenoidal foramen affects the outcome of cannulation.14 The present study shows variations in shape of foramen ovale. The maximum length of Foramen ovale on right side was 10.1mm and minimum length was 5.52mm. The mean length of foramen ovale on right side was 7.52+1.15mm. The maximum length of foramen ovale on left side was 9.7mm and minimum length was 5.43mm. The average length on left side was 7.29+1.06mm. Biswabina Ray et al.7 reported that the mean length of foramen ovale was 7.46+1.41 on right side and 7.01+1.41mm on left side. These findings of Biswabina Ray at al regarding length of foramen ovale are consistent with the findings of present study. Osunwoke et al.15 concluded that the maximum length of foramen ovale was 9.5mm and minimum length was 5mm, these findings are more or less similar to the present study. Arun SK16 reported the maximum length of about 9.8mm and minimum length of about 2.9mm. Landle MK17 stated in fluroscopically assisted laser targetting study of Foramen ovale that the average length on right side and left side was 6.9mm and 6.8 mm respectively and the average width was 3.4mm on right side and 3.8mm on left side. The findings of Arun SK17 and Landle MK17 did not matches with the present study. In the present study the maximum width of foramen ovale was 6.56mm on right side and 6.3mm on left side, whearas the minimum width of foramen ovale was 2.87mm on right side and 2.5mm on left side. The mean width of foramen ovale was 4.18+0.78mm and 4.28+0.81mm on right and left side respectively. These findings of present study regarding width of foramen ovale was found to be higher than that of other studies described by different authors. Lang J18 showed that the average length and width of foramen ovale was 7.2mm and 3.7mm on right and left side respectively. The Biswabina Ray7 stated that the average width of foramen ovale was 3.21+0.02mm on right side and 3.29+0.85mm on left side. The present study observed the ovale shaped (66.07%) foramen in majority of the skulls, this findings was in accordance of Biswabina Ray7 that reported the oval shaped foramen in 61.4% cases. Biswabina et al... found the almond shaped foramen in 34.3%, round shaped foramen in 2.9% and slit like foramen ovale in 1.4% of cases. The present study showed presence of almond shaped foramen in 32(14.28%) cases, rounded foramen in 24(10.72%) cases, D shaped foramen in 16(7.15%) and triangular shaped foramen was noticed in 4(1.78%,) of cases. Daimi SR et al.19 found oval shaped foramen in 29.87%, almond shaped in 10.41%, rounded in 12.52%, slit like in 1.04% and D shaped in 46.16% of cases. Raymond et al.10 noticed bony spur in 4.5% of cases. The study conducted by Ray et al.7 revealed that spur was present in about 3 cases. The present study shows presence of bony spur unilaterally in 4 cases. The pterygoalar bar was noticed in 5 cases by skrzat et al..14 Lepp and sander20 showed presence of osseous bridge in about 8-10% of skulls. About 7.05% unilateral and 0.89% bilateral pterygoalar bar was noticed by chouke and Hodes.21 Kapur et al.22 stated that complete unilateral pterygoalar bar was present in 5% of antolian skulls with lower frequency of bilateral pterygoalar bar. The present study revealed that the complete pterygoalar bar was found unilaterally in 7 cases whearas one skull shows incomplete presence of unilateral pterygoalar bar. Bilateral complete pterygoalar bar was found in only one skull.
CONCLUSION The present study is of clinical significance to the neurologist in cases of trigeminal neuralgia, aneurysm and in cases of diagnostic ditection of tumours when surgeon planned to approach the middle cranial fossa through foramen ovale. The present study revealed wide variations in morphometry of foramen ovale. The abnormal outgrowth like presence of bony bar, spur may lead to widespread symptoms of ischamia and necrosis.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Anatomy (Print ISSN: 2550-7621) (Online ISSN: 2636-4557) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.  This work is licensed under a Creative Commons Attribution 4.0 International License. |
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.