 Home
Home
|
Table of Content - Volume 19 Issue 2 - August 2021
Study of quadrifurcation of left coronary artery and its clinical importance
Jaishree H1, Taqdees Fatima2*, Deepalaxmi S3
1,2Assistant professor, 3Associate professor, Department of Anatomy, ESIC Dental College, Gulbarga, Karnataka, INDIA. Email: jaishreerakesh@gmail.com
Abstract Background: The aim of this study is to study the incidence of quadrifurcation of coronary artery in 76 adult human hearts using dissection method. The incidence of quadrifurcation of left coronary artery in our study is 4%. This study would be significant for proper interpretation of coronary angiographies, proper management of patient undergoing percutaneous coronary intervention as well as surgical myocardium revascularization. As coronary artery disease is one of the major cause of death in developing countries. The knowledge and incidence of such coronary artery patterns will be useful in diagnostic and therapeutic interventional procedures. Keywords: Coronary artery, Branching pattern, Quadrifurcation, Left Coronary Artery, Bifurcation
NTRODUCTION Left main coronary artery arises from left posterior aortic sinus. The initial portion of left main coronary trunk is 2 millimeters to few centimeters is and has no branches. This initial portion of left coronary artery is embedded in subepicardial fat. When it reaches the atrio-ventricular groove it divides into left anterior descending or left anterior interventricular artery and left circumflex artery. Then anterior interventricular artery produces right and left ventricular branches. The left ventricular branches vary in number from 2 to 9 and cross the anterior aspect of the left ventricle diagonally and hence known as diagonal artery.1 Usually the first diagonal artery of the is often large and may arise separately from the trunk and called as trifurcation sometimes duplicates and is called Quadrifurcation. According to Baptista et al., The Left coronary artery presented three types of division i.e Bifurcation, Trifurcation and Quadrifurcation. Bifurcation of left coronary artery branches into left anterior descending artery and left circumflex artery. In trifurcation the artery arises in between the branches of left anterior descending and left circumflex artery. The artery is named as ramus diagonals. In Quadrifurcation the two median branches were named as ramus diagonalis I and ramus diagonalis II.2 According to Suruca H.S et al. a third branch known as median or intermediate artery exists in addition to left anterior interventricular artery and left circumflex artery. 3 The artery arising between the left circumflex and left anterior descending artery is also termed as median artery by Banchi,4 Crainicianu5 named it as arterial diagnosis. Other terms used for this artery are ramus obliqus,6 ramus lateralis,7 Marginal ramus,8 intermediate artery.9 The majority of authors preferred using Ramus diagonalis which is also widely used by clinicians and physicians. Verna E et al. stated that these diagonal branches i.e ramus diagonalis have unusual anatomic course, they do not travel along the cardiac groove. They usually have a shot course and are present over the surface of the ventricle.10
MATERIALS AND METHODS This study was done on 76 adult human hearts. The specimens were collected from the cadavers during routine dissection for undergraduate medical students from Bidar institute of Medical Sciences as well as from the nearby medical colleges. By cutting the ribs and sternum, the thoracic cavity was opened, the great vessels of the heart were ligated by the thread. The heart along with great vessels were taken out of the pericardial cavity. The specimen was washed thoroughly and preserved in 10% formalin. The number of coronary arteries were noted. The origin of the left coronary artery was noted and dissected along its course, any variation in the division of main trunk of left coronary artery is noted.
RESULTS In our study the quadrifurcation left coronary artery was observed in 4% of cases.
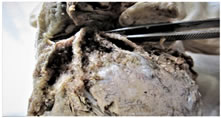
Figure 1: Quadrifurcation of coronary artery
DISCUSSION The observation of our study for incidence of quadrifurcation of left coronary artery was similar to the study done by Kalbfleisch H et al.(4.7%).6 The incidence of quadrifurcation of our study was higher when compared to the study done by Crainicianu A et al.(1%) ,5 whereas the incident was lower when compared to the studies done by Banchi et al.(13.8%) 4 and Leguerrier A et al.(7%).7 Pawel Tyczynski et al. stated that Percutaneous treatment for acute coronary syndrome of the left main coronary artery bifurcation is associated with poorer results and is complex. When additional branches arising from the left main coronary artery, percutaneous coronary intervention will be more challenging.11 According to Kosar P et al., the presence of ramus diagonalis may cause technical difficulties during coronary angiography or surgical procedures. It can also be a cause for misdiagnosis. The atherosclerosis of ramus diagonalis may have similar presentation to artherosclerosis of left anterior descending artery and left circumflex artery, as ramus diagonalis is an early branch left coronary artery.12 Galbraith et al. found that if there was a presence of ramus intermedius, it was associated with more proximal left anterior desending artery lesions which would lead to larger anterior infarctions.13 Dr Rachana Agarwal, The ramus diagonalis are described as a source of arteries supplying anterior papillary, anterior wall of left ventricle and anterior portion of septum. If the diagonal branches are absent all these areas are supplied by branches of left anterior descending and left circumflex artery. Hence in occlusion of left coronary artery and its branches more area is affected.14
CONCLUSION Almira lujinovic et al., The median branches or ramus diagonal branches along with their anastomosis they form an important way for collateral blood flow under conditions of coronary insufficiency.15 According to Venkatesan S stated that, if atherosclerosis of ramus diagonalis occurs then adjacent left anterior decending artery and left circumflex artery are also likely to be involved. Then percutaneous intervention will be very much complex.16 Since these arteries of quadrifurcation i.e ramus diagonalis are not their in their anatomical groove the procedure of stenting also becomes difficult. Hence adequate knowledge of incidence of quadrifurcation of coronary artery is important for interpretation of coronary angiography, stenting procedures and myocardial revascularisation, which would be helpful for clinicians, radiologists and physicians.
ACKNOWLEDGEMENT The authors acknowledge the scholars, whose articles are cited and used in the reference of the manuscript. Authors are also grateful to the editors/publishers of all the journals and books from where the literature is discussed and reviewed.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.