 Home
Home|
Table of Content Volume 4 Issue 2 -November 2017
Multiple renal arteries supplying the kidneys in cadavers and its clinical implications
R R Bokan1*, P B Iyer2, R M Dhappadhule3, P A Gawande4
{1Resident, Department of Anatomy} {4Resident, Department of Pathology} B. J. G. M. C. Pune, Maharashtra, INDIA. 2Professor (Additional), Department of Anatomy, Seth G.S.M.C. Mumbai, Maharashtra, INDIA. 3Resident, Department of Surgery, P. D. Hinduja Hospital Mumbai, Maharashtra, INDIA. Email: rajubokan@gmail.com
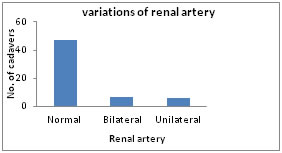
Abstract Background: The present work on renal arterial supply and its variations is undertaken because of its urosurgical importance in making a relatively bloodless surgical approach to kidneys. The advent of more conservative methods in the renal surgery has necessitated a more precise knowledge of renal vascularization and its importance in partial and total renal transplantation surgeries. Aim: The aim of this study is to recordthe variation in the site of origin of renal arteries in human cadavers. Objective: To record the variations of arteries supplying the kidneys in cadavers. Materials and Methods: Sixty cadavers embalmed with 10% formalin were utilized in this study. Variations in the origin of the renal arteries were noted. Results: It was observed that the out of 60 cadavers, the renal artery showed variations in 13 of them [21.66%]. Seven cadavers had variation bilaterally and six cadavers unilaterally, three from right side and three from left Side. The knowledge of variations of the renal arteries forms an essential guide line for urosurgeons during partial and total renal transplantation surgeries. Attemptismadeto discuss the embryological and clinical significance of the multiple renalarteries. Key Words: Embryology, Renalarteries, Urosurgeon.
The renal vasculature was originally recognized by John Hunter, who, in 1794 wrote “the veins in the spleen and kidney anastomoses in very large trunks while the arteries do not at all” 1. Renal arteries supply the kidneys through a number of subdivisions described sequentially as segmental lobar, inter lobar, and arcuate arteries. The segmental arteries are end arteries with no anastomoses. The arcuate arteries further divide into interlobar arteries, which give rise to the afferent arteries of glomeruli. The renal arteries branch laterally from the aorta just below the origin of the superior mesenteric artery. Accessory renal arteries are common and exist in 30% of individuals, and usually arise from the aorta above or below the main renal artery and follow it to the renal hilum. They are regarded as persistent embryonic lateral splanchnic arteries. Rarely, accessory renal arteries arise from the coeliac or superior mesenteric arteries near bifurcation or from the common iliac arteries 3. Development: The lateral splanchnic arteries arise from the abdominal part of the developing aorta supply the structures developing in whole or in part from intermediate cell mass i.e., the suprarenal gland, the kidney and the gonads (ovary or testis).These arteries are well developed only in the regions of developing pronephos, mesonephros, and metanephros. They form irregular series of vessels in the adult (rete arteriourogenitale).Presumably in the primitive condition, there was a pair in each segment of the body but many of them disappear and the series is represented in the adult only as the suprarenal, the renal and gonadal arteries possibly also by some of the branches of the internal iliac artery. During the development of mesonephros, nearly 18-20 pairs of these vessels arise from the aorta but, most of them disappear, only one gonadal artery and three suprarenal arteries persist on each side. The phrenic artery branches from the most cranial suprarenal artery and the definitive renal artery arise from the most caudal. Additional renal arteries may frequently be present and may be looked on as the branches of persistent lateral splanchnic arteries. The kidney is originally at the level of upper sacral segment and receives its early arterial supply from the lateral sacral branches of the aorta. The ascent of kidney from its original pelvic region to its final lumbar position takes place between the ends of 5th week and 8th week. During the ascent of kidney, their intrinsic blood vessels receive their blood supply from the lateral stem arteries, which arise from the aorta at increasingly higher level until that definitive renal arteries, at the second lumbar vertebra is reached. This definitive renal artery is the most caudal of three suprarenal arteries. This artery, now called as renal artery, supplies the kidney and inferior surface of suprarenal gland3. The first anatomical findings on the renal artery, and the fact that one kidney can be provided with more than one renal artery, were shown by Eustachius in 1552, in anatomy illustrations engraved in copper. Since then, until today, the vascularization kidney has been researched, with the special attention paid to variations in the arterial supply of this organ. Different terms have been used, such as: abnormal blood vessels, accessory, extra-hilar, multiple or aberrant blood vessels. All this creates a statistical gap in terms of their accurate type, number and the point of separation (parting point).Accessory arteries though called accessory are essential to a particular segment of the kidney as ligature of these arteries results in ischemia to the particular segment. Studies on accessory arteries not only include the percentage of them present in the population but also the number of arteries on the both sides. Owing to the urosurgical importance of making a relatively bloodless surgical approach to kidneys as well as embryological basis of variations in the vascular supply of the kidneys, this study is undertaken with the following objectives:
MATERIAL AND METHODS Cadavers were obtained from a teaching institute and tertiary care hospital. Out of 60, 55 cadavers were of males and 5 cadavers were of females. All the cadavers were ranging between the age group of 18-65 years. None of the cadavers showed any evidence of previous surgery.With due permission of Ethics committee (after getting NOC) renal artery was dissected in formalin fixed 30+30=60 cadavers and 120 sites were utilised. Damaged and horseshoe kidneys are excluded from the study.10% Formalin solution used as a preservative for the specimen. Dissection was carried out in the following manner.The abdomen was opened by a midline incision extending from xiphoid process to pubic symphysis. The peritoneum and intestines were retracted and kidneys exposed. Peritoneal organs were removed systematically till exposure of the kidneys. Peritoneum, renal fascia and fat were cleared off from the kidneys and the arteries followed from their origin to the renal hilum. Renal veins, fat, and connective tissue were gently removed to expose the entire abdominalaorta and renal arteries, and additionalrenalarteries and then data were recorded and compiled and analysed statistically.
Figure 1: Showing variations of renal artery Figure 1: Figure 2:
Figure 3: Figure 4:
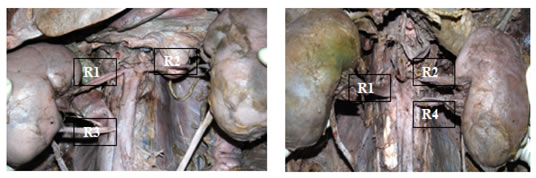
Figure 5: Figure 6: Figure 1: Normal renal vasculature; Figure 2: Bilateral double renal arteries; Figure 3: Right side double renal arteries; Figure 4: Left side triple renal arteries; Figure 5: Right side double renal arteries; Figure 6: Left side double renal arteries R1-Right side renal arteries , R2 - Left side renal arteries, R3-Right side additional renal arteries, R4 - Left side additional renal arteries, R5 - Left side additional renal arteries DISCUSSION The variations in the renal arteries are mainly due to the various developmental positions of the kidney. Different origin of renal arteries and their frequent variations are explained by the development of mesonephric arteries. Early ramification of the main renal artery as observed in our study was, such a morphological expression is important due to these branches being erroneously interpreted as additional arteries in diagnostic imaging studies and has surgical complications in renal transplants; since the first 15 mm of the renal artery can be used for anastomosis with the recipient’s iliac artery. It should also be emphasised that early ramification of the main renal artery and the presence of additional arteries represent exclusion criteria in laparoscopic renal surgery. According to David Sykes, when there were many accessory renal arteries, the superior accessory artery is a separate segmental artery and the inferior accessory artery is a separate lower segmental artery2. Additional arteries are frequently found in renal vascular irrigation studies. The frequency observed in study of the Colombian population (24.9%), Indian population (13.5%), mestizo population (18.5%), the Thailandese (17%) and black populations (18%). Studies on Caucasian and black populations have reported frequencies ranging from 30% to 40%.The differences in additional artery frequency may have been due to ethnic factors, the type of study or the evaluated sample’s size2. In present study from 60 cadavers 13 cadavers were found variation in renal artery (21.66%), of them Seven cadavers had variation bilaterally (11.7%) and six cadavers unilaterally (10%), Three from right side and Three from left Side. Robert J Merklin and Nicholas A Michels reported various possibilities of origin of segmental renal arteries from inferior phrenic artery to apical or upper segmental, apical artery giving rise to inferior suprarenal artery, and origin of upper, middle or lower segmental arising directly from abdominal aorta11. Patel Shashikala, Wanjari Anjali et al, showed case unilateral left double renal artery in 54-year- old male cadaver during routine dissection of abdomen. First renal artery (RA) arose from aorta at the level of L1 vertebra, whereas 2nd renal artery arose from same 5 cm below to the first one. Both RA ran laterally and entered the kidney through the hilum with their anterior and posterior divisions 13. Embryological explanation of these variations has been presented and discussed by Felix. In an 18mm foetus, the developing mesonephros, metanephros, suprarenal glands are supplied by nine pairs of lateral mesonephric arteries arising from the dorsal aorta. Flex divided these arteries into three groups as follows: 1st and 2nd arteries as the cranial, 3rd to 5th arteries as the middle group, and the 6th to 9th arteriesas the caudal group. Persistence of more than one artery of middle group results in multiple renal arteries. Thus the multiple renal arteries in present study due of persistence of lateral mesonephric arteries from the middle group14.
Table 2: Variation of Renal artery compared with other studies
CONCLUSION The anatomical variations, studied by numerous authors, are found in apparently normal individuals. In the present study, we observed six cadavers with three renal arteries, which represent 10% of the total of cadavers, six cadavers with four renal arteries, which represents 10% of the total of cadavers and one cadaver with five renal arteries, which represents 1.6% of the total of cadavers. The description and the knowledge of existing variations in renal arteries, help to plan and carry out safer surgical interventions, optimizing the process and reducing the risk of death of patients.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.