 Home
Home|
Table of Content Volume 5 Issue 1 - January 2018
Study of suprascapular notch and its variants
Varsha P Dahiphale1, Satishkumar S Porwal2*, Shankar S Dhapate3
1Associate Professor, 2Assistant Professor, 3Professor and HOD, Department of Anatomy, S.R.T.R. Government Medical College, Ambajogai-431517, Dist.-Beed. Maharashtra, INDIA. Email: satish27181@yahoo.co.in
Abstract Background and Aims: The suprascapularnotch (SSN) is a variable depression on the superior border of scapula medial to the base of the coracoid process. The shape and size of suprascapular notch is one of the most important risk factor in suprascapular nerve entrapment. The suprascapular nerve entrapment can occur at the suprascapular notch or at the spinoglenoid notch. Better knowledge of the suprascapularnoch anatomy may help to prevent and to assess more accurately suprascapular nerve entrapment syndrome. Aim of the present study was to assess morphology and morphometry of SSN and correlate the findings with the risk of nerve entrapment. Material and Methods: A total 161 adult human scapulae obtained from various medical colleges of marathwada region of Maharashtra. Various shapes of SSN observed were photographed and classified. Various parameters of SSN measured by using digital verniercaliper. Results: Various shapes of SSN observed were mere a depression, ‘U’, ‘V’, suprascapular foramen and SSN with foramen. There are more chances of nerve entrapment with ‘V’ shaped nocth. Conclusions: The morphology and morphometric knowledge of SSN is essential to suspect suprascapular nerve entrapment as one of the cause of shoulder pain and weakness in shoulder movement. It is also helpful to prevent iatrogenic injury to suprascapular nerve during surgical procedures of shoulder region. Key Words: Scapula, Suprascapular nerve entrapment, Suprascapular notch, variations.
The suprascapular notch is a variable depression on the superior border of scapula medial to the base of the coracoids process. The superior transverse scapular ligament (STSL) bridges over the notch and converts the notch into the passage to allow the passage of suprascapular nerve to supraspinatus fossa1. Occasionally a bony ridge resulting from the ossification of the ligament may form and convert the notch into the foramen (SSF). This occurrence is frequently seen in animals, but its prevalence is said to be very low in humans2. Suprascapular nerve supplies motor branches to supraspinatus and infraspinatus muscle, sensory branches to rotator cuff muscles and ligaments of shoulder joint and acromioclavicular joint. This notch is important landmark of the suprascapular nerve during arthroscopic shoulder operations3. Anatomical variations in morphology of suprascapular notch and the anomalous or ossified superior transverse scapular ligament are considered to be risk factor for suprascapular neuropathy4. Rengachary et al classified suprascapular notch into six types based on its shape5,6. Type I: The superior border of scapula presents a depression from the medial superior angle to base of coracoid process. Type II: A wide blunted “V” shaped notch occupying nearly a third of the superior border with the widest point along the superior border. Type III: A symmetric and “U” shaped notch. Type IV: A very small “v” shaped notch Type V: Similar to type III with partial ossification of the medial border of the notch and with minimum diameter of along the superior border of scapula. Type VI: A bony foramen with completely ossified STSL The shape and size of the suprascapular notch is the most important factor in aetiopathology of suprascapular nerve entrapment. A narrow suprascapular notch may predispose a patient this neuropathy. Also a V-shaped notch is more likely to be associated with nerve entrapment5. Therefore knowledge of the suprascapular region especially suprascapular notch and superior transverse suprascapular ligament and its variations is particularly important in various techniques associated with arthroscopic suprascapular nerve decopmpression5. The present study deals with morphology of suprascapular notch and specific geometrical parameters of suprascapular notch which describe almost all variations of suprascapular notch and comparison with the study of previous workers.
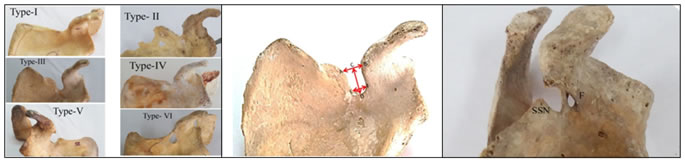
MATERIAL AND METHODS A total 161 adult human scapulae obtained from various medical colleges of marathwada region. Damaged/broken Scapulae were excluded from the study. Photographs of the various types of suprascapular notch were taken by using digital camera. The suprascapular notches in scapulae were classified based on the classification of Rengachary et al (Fig. 1). Various measurements of suprascapular notch were taken by using digital vernier calliper. The following parameters were taken (fig.2)
AB-Upper transverse diameter, EF-Lower transverse diameter, CD-Vertical diameter In the scapulae where notch was absent (Type-I) and those with a suprascapular foramen the measurements were not recorded. OBSERVATION AND RESULTS Based on Rengachary classification the frequencies of the various types of suprascapular notches were observed in the present study were as follows:
Table 1: Showing frequencies of various types of SSN
Above table shows that frequency of occurrence of type I, II, III, IV, V and VI SSN was 74,11,40, 6,21 and 8 scapulae respectively. Also it shows that, ‘U’ shaped SSN (Type III and V) was observed in 61 scapulae and ‘V’ shaped SSN (Type II and IV) was observed in 17 scapulae. Complete ossification of suprascapular ligament that is suprascapular foramen was observed in 8 scapulae. Coexistence of suprascapular notch and suprascapular foramen is the rare osteological anomaly in the scapula, in which a bony lamina intervenes between these two bony landmarks. In the present study one scapula showed presence of foramen along the inferolateral side of SSN (fig.3).
Figure 1 Figure 2 Figure 3 Legend Figure 1: Anterior view of scapula showing types of suprascapular notches based on Rengachary classification; Figure 2: Anterior view of left scapula showing various measurements of SSN; Figure 3: Anterior view of left scapula showing suprascapular notch and foramen SSN-Suprascapular notch, F- Foramen
Table 2: Showing mean upper transverse diameter of various types of suprascapular notches
Table 3: Showing mean lower transverse diameter of various types of suprascapular notches
Table 4: Showing mean vertical diameter of various types of suprascapular notches
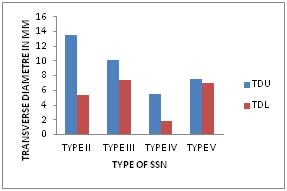
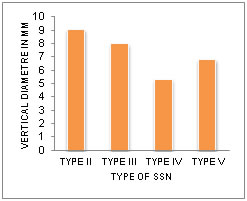
Figure 1 Figure 2 Legend Figure 1: Showing comparison of mean transverse diameters of different types of suprascapular notches at upper (TDU) and lower(TDL) levels of SSN Figure 2: Showing comparison of mean vertical diameter of different types of suprascapular notches DISCUSSION Several descriptions of the suprascapular notch variations have been studied in different populations by Hradicka, Olivier, Rengacharyet all, Natsis et all, Sinkeet, vangang7. Rengachary et al5,6 classified the suprascapular notch into six types based on its shape. In the present study type I- SSN was more common followed by Type III, V, II, VI and IV. The least common type of SSN was Type IV. Also, the presence of both SSN and suprascapular foramina was observed in one scapula (0.62%).These findings were not similar to that of other studies. In the studies of other authors Type III- SSN was more common. Table 5: Showing Comparison of frequencies of various types of SSN by Rengachary
Table no.5 Indicates that, the findings of the present study are near to the findings with the Sinkeet et al (Kenya) and Muralidhar et al (India). Incidences of various SSN were different in different populations. SN Badagabettu et al(2014) reported a case of presence of suprascapular foramina(SSF) along with the SSN as that of the present study9. The coexistence of SSN and SSF is a very rare condition. Very few such case have been reported so far. The frequency of coexistence of SSN and SSF is variable depending on the group of populations. It was found that its occurrence is 0.33% in Polish population and about 0.7% in German and Kenyan populations9. In the present study occurance of coexistence SSN with suprascapular foramen was similar to that of German and Kenyan population. Michael et al in their case series studies have described four hypothetical possibilities of the formation of bony bridge separating SSN from the SSF making the coexistence of SSN and SSF9:
Morphological alteration in SSN or SSF are undoubtedly the predisposing factors for the suprascapular nerve entrapment. Coexistence of the SSN and SSF as seen in the present study increases the risk of neuropathy by causing nerve irritation against bony margins during its passage through the foramen. In the present study the difference between mean of upper and lower transverse diameter is more in V shaped notches that is Type II and IV which is 8.12mm and 3.3mm respectively as compared with U shaped notches that is Type III and V which was 2.6mm (T.III) and 0.22mm(T.V) (Table no. 2, 3 and Graph no.1). This showed that U shaped notch had a large area than the V shaped notches, leading to an assumption that V shaped notch was more likely to be concerned with the nerve entrapment. Vertical diameter of Type II (Large ‘V’) was more than that of Type IV (small ‘v’). This indicates that type IV SSN was more prone for nerve entrapment (Table no. 4 and Graph no.2). In the present study the U shaped notch (37.88%) was more common than the V shaped notch (10.50%) similar to the previous studies (Table no. 1).
Table 6: Showing comparison of Distribution of U and V type of notch in different populations
The complete ossification of STSL could have basically a genetic influence. Cohen et al described a familiar case of calcification of STSL affecting the 58 yrs old man and his son causing suprascapular nerve entrapment syndrome with a symptomatic involvement of supraspinatus muscle with complaints pain and weakness in shoulder4. Anatomical variations of the anterior coraco-scapular ligament as well as the existence of a bifid or trifid STSL, that are important anatomical factors influencing type of notch and the incidence of the suprascapular nerve entrapment syndrome.4. In the present study incidence of complete ossification of STSL (4.96%) was similar with that of Rengachary (4%).
CONCLUSIONS The knowledge of variants of suprascapular notch is essential in patients with shoulder disorders since suprascapular nerve entrapment as one of the cause. The knowledge of normal anatomy of suprascapular notch and its variants is helpful in surgical procedures of shoulder region to avoid iatrogenic injury to suprascapular nerve.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.