 Home
Home|
Table of Content Volume 5 Issue 2 - February 2018
Variation associated with non-piercing of coracobrachialis by musculocutaneous nerve
John P Sneha1, Meenakshi P Borkar2*, Mehera M Bhoir3
1Registrar, 2Assistant Professor, 3Professor and HOD, Department of Anatomy, HBTMC and Dr. R N Cooper Municipal General Hospital, Mumbai, Maharashtra, INDIA. Email: drmeenakshiukey@gmail.com
Abstract Background: The Musculocutaneous nerve is the branch of lateral cord of the brachial plexus. It then passes laterally and pierces coracobrachialis. After piercing coracobrachialis it descend laterally between biceps and lateral side of the arm to continue as lateral cutaneous nerve of the forearm. Commonly musculucutaneous nerve shows variation in origin, course, branches, termination and it's connections with other nerves of brachial plexus. These variations have clinical significance during surgical procedures, in the brachial plexus block and in diagnostic clinical neurophysiology. It is important to be aware of this variation while planning the surgery in the region of the arm, as these nerves are more liable to be injured during the operation. Methods: A comprehensive study was carried out on 48 limbs by using 24 embalmed cadavers. Dissection of infraclavicular part of brachial plexus was done. The variation in the origin, number and course and their correlations to the coracobrachialis were noted. Results: The Musculocutaneous nerve didnot pierce coracobrachialis in 2 of the limbs. Key Words: Musculocutaneous nerve, Coracobrachialis, Biceps brachii, Axillary artery.
The musculocutaneous nerve arises from the lateral cord (C5-C7), opposite the lower border of pectoralis minor. It pierces coracobrachialis and descends laterally between biceps and brachialis to the lateral side of the arm. Just below the elbow it pierces the deep fascia lateral to the tendon of biceps, and continues as the lateral cutaneous nerve of the forearm. A line drawn from the lateral side of the third part of the axillary artery across coracobrachialis and biceps to the lateral side of the biceps tendon is a surface projection for the nerve (but this varies according to its point of entry into coracobrachialis). It supplies coracobrachialis, both heads of biceps and most of brachialis after piercing coracobrachialis. The branch to brachialis also supplies the elbow joint. A small branch to humerus enters the shaft with the nutrient artery1. The fibres of the musculucutaneous nerve are from the seventh cervical ramus and may branch directly from the lateral cord.
MATERIAL AND METHODS Forty eight upper limbs from twenty four adult cadavers we're utilized for the study during 3 years. Origin and branches of musculocutaneous nerve were studied and relation of nerve with coracobrachialis muscle was noted.
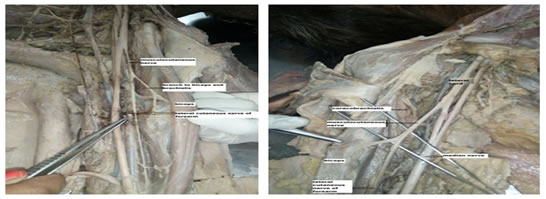
OBSERVATIONS In two out of forty eight upper limbs Musculucutaneous nerve were not piercing coracobrachialis muscle. Forty eight upper limb were meticulously dissected, out of which two cases showed variation. In the first case variation was noted in left upper limb. It arised from the lateral cord at the upper part of the coracobrachialis muscle. After this it divided into two branches. One branch was given to coracobrachialis, biceps and brachii and other branch continued as lateral cutaneous nerve of the forearm. (Fig no 1). Similar case was noted in right upper limb. (Fig no 2).
DISCUSSION The musculocutanoeus nerve is a mixed nerve of the upper limb. The anterior compartment of the arm is supplied by the motor component of the musculocutaneous nerve. It innervates coracobrachialis, biceps and the brachialis. Lateral cutaneous nerve of the forearm is the sensory part of the musculocutaneous nerve. It innervates skin on the lateral side of the forearm. In present study 4.16 % of the cases, the musculocutaneous nerve didnot pierce the coracobrachialis. The present variation coincides with D. Jagadeeshbabu, P.D. Sonje, Chitra, Sachdeva K et al. D. Jagadeesh Babu2conducted a detailed study on 50 upper limbs by using 25 embalmed cadavers. Dissection on the infraclavicular part of the brachial plexus showed variations in the origin of musculocutaneous nerve. The nerve was found to be not piercing coracobrachialis in 2 of the limbs and it coincides with the present study. Dr. P.D. Sonje3 in his study had four types of observation about variations of musculocutaneous nerve Type 1 – Non piercing of coracobrachialis and having two communicating branches with median nerve. Type 2 – Non piercing of coracobrachialis without communication with median nerve. Type 3 – Piercing coracobrachialis muscle having two communicating branches with median nerve. Type 4- Non piercing coracobrachialis and having one communicating branch with median nerve. Type 2 coincides with the present study. M Jamuna et al4 reported in their study that the musculocutaneous nerve was found to be absent completely in 3 limbs. Sachdeva K. and Singla RK5 found that musculocutaneous nerve was not piercing the coracobrachialis muscle and then branches to the biceps brachii and brachialis muscle were given. Dr Girish V. Patil and Dr Shishirkumar6found musculocutaneous nerve without piercing coracobrachialis muscle passed along the medial aspect of muscles of arm. P.V.V. PrasadaRao7, reported out of 24 upper limbs dissected, the musculocutaneous nerve was found to be absent in 8% of the cases. In a routine dissection of a 79-year-old male cadaver Marwan F et al 8 found a unilateral three-headed biceps brachii muscle coinciding with an unusual variant of the musculocutaneous nerve. In a routine dissection, in 60 yr old male cadaver Muhammad saed et al 9 noticed an unusual formation of the median and musculocutaneous nerve.
CONCLUSION Musculocutaneous nerve injury alone is very rare. It may occur if there is injuries to shoulder and upper arm. For example in fracture of humerus or in patients with neuralgic amytrophy. As musculocutaneous nerve supplies biceps brachii and brachialis, injury to nerve may cause paralyses of these muscles, which may manifest as marked weakness of elbow flexion. It may be associated with loss of sensation on the extensor part of the forearm. Pain and paraesthesia may be aggravated by elbow extension. The observations in the study show that musculocutaneous nerve has notable variations. Knowledge about these variations is important to avoid complications during surgical reconstructive procedure. For e.g. arthroplasty in recurrent shoulder dislocation, in arthroscopy of shoulder joint, repair of fractures of humerus, performing nerve transfer procedures of Brachial plexus, in brachial plexus blocks, so that these structures can be identified and protected. It is important for surgeons, clinicians and anatomists.
Figure 1 Figure 2 Legend Figure 1: Musculocutaneous nerve not piercing coracobrachialis and dividing into branches in left upper limb. Lateral branch supplies biceps and brachialis. Medial branch continous as lateral cutaneous nerve of forearm. Figure 2: Musculocutaneous nerve not piercing coracobrachialisin right upper limb REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.