 Home
Home|
Table of Content Volume 6 Issue 1 - April 2018
Study of caudate lobe of liver in dissected cadaveric liver specimen
Anju Balaji More1*, Balaji Dagadu More2
1Associate Professor, Department of Anatomy, Maharashtra Institute of Medical Sciences and Research, Latur, Maharashtra-413512, INDIA. 2Clinical Pharmacologist, Latur, Maharashtra-413512, INDIA. Email: as.anju@yahoo.in
Abstract The study was planned to study the portal vessels in relation to caudate lobe of the liver specimen without any liver pathology obtained by cadaveric dissection. It is a study of pattern of portal vein supply to caudate lobe using cadaveric liver specimen preserved in formalin. Study also includes morphologic and biometric of inferior vena cava, main portal vein and its two main tributaries. Left portal vein supply to right portion of caudate lobe (64%) and left portion of caudate lobe (100%) of the total specimen studied. Caudate process has always received its blood supply from right branch of portal vein. The main portal vein terminates by dividing into right and left portal vein in majority of specimen. If segmental veins arise as direct branches of main trunk, either of the branches are absent. The internal and external diameter of Inferior vena cava, main portal vein and its right and left tributary has been measured. Study of Pattern of portal vessels by dissection tells about different arrangements and range of dimensions of these vessels. It aids to define segments and their respectability prior to surgery. Key Words: Caudate (Spigelian) lobe, Caudate process, Portal vein, Liver.
INTRODUCTION The caudate lobe (posterior hepatic segment I, Spigelian lobe) is situated upon the postero-superior surface of the liver on the right lobe of the liver, opposite T10-11. The boundaries are ligamentum venosum on leftside; the porta-hepatis below and Inferior vena cava (IVC) on the right.1 It separates fossa for gall-bladder from that of IVC. Its right oblique lateral extension at lower border is called caudate process. Occlusion of hepatic venous outflow in Budd-Chiari syndrome, can lead to its hypertrophy.2 The caudate lobe is supplied by left portal vein. Its paracaval portion receive its blood supply from main portal vein and its bifurcation whereas caudate process from right portal vein. The blood from caudate lobe is drained by one or more hepatic veins. Knowledge of the biometrics of portal veins defines surgical anatomy of the caudate lobe.3,4
MATERIAL AND METHODS The study was conducted in the Department of Anatomy at Seth GS Medical College and KEM Hospital, Parel, Mumbai-12. It was an observational study. Grossly normal cadaveric livers were obtained from cadavers preserved by embalming them in 10% formalin for routine undergraduate dissection. The livers dissected as a specimen after ‘Abdomen dissection’ was obtained with prior permission of Head of the Department. The liver was dissected and removed from its location by cutting all the peritoneal attachments. 5o liver specimen free from any gross evidence of cirrhosis, abscess, primary and secondary malignancy were included in the study. These were stored in 50% formalin. The container used was sufficient to avoid mechanical damage to the liver specimen. Dissection of cadaveric liver: The finger fracture technique suggested for liver dissection during surgery is used. Each liver is dissected into four sectors by dividing the liver tissue by finger dissection along the plane of three major hepatic veins. The blunt end of knife was used to tease away the liver parenchyma and expose vessels. The middle hepatic vein (MHV) lies along cantile’s plane. So, the vessels can be exposed if the parenchyma is dissected along the plane passing from the left side of Inferior Vena Cava (IVC) to the middle of gall bladder fossa. This plane separates right lobe from the left. The vessel was traced from its confluence into the IVC further to show its tributaries. The liver tissue was teased away to expose it. Right hepatic vein (RHV) lies along right scissura, which divide the right lobe into anterior and posterior segments. The left hepatic vein (LHV) lies within the left lobe; occupies and forms the left intersegmental plane. It is first traced from its confluence into the IVC. The caudal part of the plane is demarcated by umbilical fissure containing the left portal vein (LPV). This plane divides the medial segment from the lateral segment of left lobe. These veins occasionally unite before they terminate into IVC exhibiting various patterns. The diameter is measured within 1cm of their confluence into the IVC. The diameter of IVC is measured in the infra diaphragmatic part at the superior surface of the liver. Dividing the liver along the planes of portal vein and its branches offers further dissection of liver into segments. The main portal vein enters the liver substance at the porta hepatis. It divides into right and left portal veins. These branches are seen when the connective tissue and the lymph nodes at the porta hepatis are removed. The right portal vein traverses to the right and divides into anterior and posterior segmental branches. Occasionally they are direct branches of the main portal vein. These are dissected by teasing away the hepatic tissue by blunt end of knife. The diameter of the vessels was measured using the divider and scale, as in fig 1 and 2. The vessel is cut at its formation. The diameter is measured along two planes perpendicular to each other and their mean is taken. The external diameter was measured in 50 where as the internal diameter was measured in only 20 livers. As these intersegmental fissures are dissected, the caudate lobe is separated from rest of the liver tissue along its boundaries. Disposal of dissected liver: The dissected specimens were preserved in 50% formalin solution. With due respect to the biological specimens the livers were disposed off by cremation at the Panvel centre. Analysis of data: Data was analysed by using statistical tests: mean and standard deviation. Ethics committee approval: The study was carried out after the approval of Institutional ethics committee.
DISCUSSION Liver Anatomy: The liver is a vital and complex gland, with a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion. It has two distinct descriptions, according to its morphological and functional aspects. Morphologically the liver presents 4 lobes: left, right, caudate and quadrate. Functionally the liver present a different anatomy, and one of the proposed ones is the Couinaud model, which is used within this work. The functional anatomy model of Couinaud proposes the division of the liver into eight different regions according to the portal and hepatic veins positions: Segment I - caudate/Spiegel lobe Segment II - left posterolateral Segment III - left anterolateral Segment IVa - left superomedial Segment IVb - left inferomedial Segment V - right anteroinferior Segment VI - right posteroinferior Segment VII - right posterosuperior and Segment VIII - right anterosuperior5,6 As illustrated in figure 3, each segment has its limits defined by the hepatic veins and the portal vein, except segment I, which is drained by the IVC. The observations of the study indicate that the internal architecture of the liver varies. The portal vein branches feed the segments where as hepatic veins lie in the intersegmental plane. The number of segments is consistent i.e. eight. To equate the segments described with their differing names and the limitations, quoted by all the investigators would not improve the reliability of the information towards its practical application. Because it is the vessels defining the segments, whose morphology and biometry matters during imaging and surgery, the study consist of study of these vessels.7 Caudate lobe receives its blood supply along with hepatic artery; from portal vein and its tributaries. Left branch of portal vein supply right portion of caudate lobe in 64% and left portion in all specimen. Right portal vein supply to caudate process in the entire 50 specimen studied and right portion of caudate lobe in 9 specimen. Main trunk of portal vein do not supply to caudate process and left portion of caudate lobe. (Table 1) Table 1: Mode of blood supply of caudate lobe
Table 2: Patterns of division of main portal vein
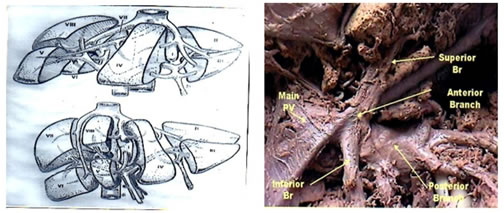
The incidence of absence of right portal vein due to origin of segmental veins as direct tributaries of main portal vein has been noted in 8% of cases as compared to 12% by Gupta et al. (Table 2) Right portal vein is absent if portal vein directly divide into segmental veins. In figure 4 shows main portal vein branching into subsegmental branches; superior and inferior branch of anterior trunk and posterior trunk (branches of right portal vein). Left portal vein (LPV) gives horizontal and ascending segmental veins. Horizontal segmental vein of LPV lie anterior to caudate lobe separating caudate lobe posteriorly from medial segment of left lobe anteriorly. Ascending segmental vein of LPV divides medial from lateral segment of left lobe.
Table 3: Measurements of diameter
The internal and external diameter of major vessels gives information about its calibre and thickness of vessel wall. Mean external diameter of Inferior vena cava is 21.61mm. The mean internal diameter of main portal vein is 14.6mm. (Table 3) Figure 1: Figure 2:
Figure 3: Figure 4: Figure 1: Measurement of internal diameter Figure 2: Measurement Figure 3: Vascular Segments of liver Figure 4: Main portal vein dividing into subsegmental branches
CONCLUSION The anatomy of the caudate lobe has surgical relevance for resection of both the patient as well as donor.8 In hepatocellular carcinoma (primary and metastatic tumors) and hilar bile duct cancer, partial or total caudate lobectomy is often necessary for complete extirpation of the tumor. The caudate lobe is resected from donor’s liver in preparation for living related donor transplantation. The significance is reflected in the increase in frequency and safety of its resection.9,10 This section of liver is embryonically and anatomically independent of the right and left liver and the main portal fissure. The caudate lobe is in contact with the vena cava, except at the entrance of the main hepatic veins into the vena cava. The entire caudate lobe is a single anatomic segment that is defined by the presence of portal venous branches. The diameter and area of supply of main portal vein and its tributaries decide the course of surgery during transplantation.11,12 The transplantation and resection of liver are in their initial stages in India. So, such data is not available in Indian population. Individual variations in morphology of vessels exist. Knowledge of vessels will define the caudate segment of liver. It helps to plan the plane of resection for surgeries helping in conservation of normal tissue.13 Palliative embolisation of portal vein feeding the affected segment may provide some relief to the patient14
ACKNOWLEDGEMENT The present article is part of dissertation submitted for the degree of M.S. (Anatomy) of the University of Mumbai. I would like to express my sincere gratitude to my respected Guide and my present Institution: Maharashtra Institute of Medical science and Research, Latur.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.