 Home
Home|
Table of Content Volume 6 Issue 3 - June 2018
Variations in carotico clinoid foramen in human skulls in western Maharashtra region and its clinical significance
Pallavi A Kulkarni1*, Avinash D Shewale2, Rohini R Karambelkar3
1Associate Professor, Department of Anatomy, SKN Medical College and General Hospital, Pune, Maharashtra, INDIA. 2Associate Professor, Department of Anatomy, Yogita Dental College, khed, Chiplun, Dist. Ratnagiri, Maharashtra, INDIA. 6Professor, Department of Anatomy, Prakash Institute of Medical Sciences and Research, Islampur, Dist. Sangli, Maharashtra, INDIA. Email: pakulkarni57@gmail.com
Abstract The lesser wing of sphenoid bone ends medially as anterior clinoid process (ACP), excision of anterior clinoid process is needed for exposure of clinoid segment of internal carotid artery, expose cavernous sinus and to manage paraclinoid aneurysm. ACP is connected to middle clinoid process by ligament known as carotico clinoid ligament (CCL) which may be ossified forming carotico clinoid foramen (CCF). Sometimes CCL is ossified and may have compressive effect on internal carotid artery. Anatomical knowledge about the dimensions of CCF may be useful in cases of surgery involving removal of ACP. In the present study, eighty two human dried skulls of known sex were studied. It has been observed that the incidence of presence of CCF is 28%; among which CCF was observed more on right side as compared to left side. When CCF was analysed for diameter, sexual variation was observed but, it was not statistically significant. When CCF is present, it is likely to compress internal carotid artery and also cause morphological changes in internal carotid artery. When calibre of internal carotid artery is more than the diameter of CCF there is high possibility of inducing a headache caused by compression of internal carotid artery. The position of CCF is in area close to cavernous sinus. The formation of CCF may change the dimensions of cavernous sinus. Anatomical knowledge of the dimensions of the carotico clinoid foramen may be useful in cases of surgery involving removal of anterior clinoid process. Key Words: ACP, CCF, CCL, Human skull.
INTRODUCTION Sphenoid bone is wedged between the frontal, temporal and occipital bones at the base of the skull. It has a central body, paired greater and lesser wings spreading laterally from it and two pterygoid processes descending from the junction of body and greater wings. The lesser wings end medially as ‘anterior clinoid process’. It provides attachment to anterior end of free border of tentorium cerebelli. Anterior boundary of sellaturcica is completed laterally by two small eminences called ‘middle clinoid process’. The super lateral angles of dorsum sellae end in two tubercles of varying sizes ‘ posterior clinoid process’. It gives attachment to the attached marginof tentorium cerebelli. (Gray’s Anatomy) The anterior clinoid process is joined to the middle clinoid process by the carotico clinoid ligament which is sometimes ossified. A dural fold extending between the anterior and middle clinoid processes or ossification of the carotico clinoid ligament, may result in the formation of the ‘carotico clinoid foramen’. The interclionoid ligaments connect the anterior clinoid and posterior clinoid processes. Sometimes the interclinoid processes also get ossified and that is called as ‘sellar bridges’. The caratico clinoid foramen andsellar bridges may be unilateral or bilateral. The caratico clinoid foramen is an inconstant structure which is located in middle cranial fossa, composed by the ossification of the fibrous ligament17 that begins at the anterior clinoid process andjoins the middle clinoid process6. Carotico clinoid foramen allows the passage of one of the segments of the internal carotid artery, the clinoid segment.6,17. Several authors studied the anatomical characteristic of carotico clinoid foramen in different populations.4,12,14. Due to its location on the skull these characteristics associate to clinical importance which is considered of great interest for neuroanatomyand neurosurgery2,3,8,16. Knowledge about the ossification of carotico clinoid ligament is important in the neurosurgical operations. The anterior clinoid process is usually accessed in order to gain entry into the clinoid space10. After the internal carotid artery leaves the cavernous the sinus, it is related medially to the anterior clinoid process. The presence of an ossified carotico clinoid ligament may form a potential site for compression of the internal carotid atery10. The aim of present study is to evaluate the incidence of skulls with the carotico clinoid foramen as well to perform it morphometryand clinical influences generated by these structures.
MATERIAL AND METHODS In the present study, total 82 adult dried Human Skulls of known sex (50 Males and 32 Females) belonging to dept. of anatomy were taken for investigation. To select the skulls, integrity of the clinoid process was checked. Three with damaged clinoid process were excluded from the study. A selection criterion for skulls was with at least presence of one catotico clinoid foramen with complete ossification of fibrous ligament on unilateral or bilateral side. The incidence according to the sex was also considered. The morphometric was performed using a manual calliper tomeasurethe major diameter of each foramen. To avoid errors, the measurements were performed three times by the sameresearcher considering the repeated values. These values were obtained in millimetre. Statistical analysis was done after tabulating the values.
Table 1: Morphometry results for CCL
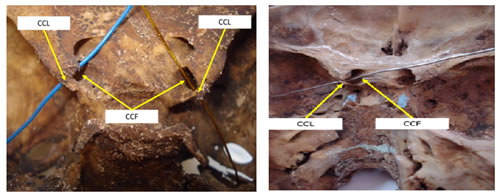
Measurements of CCL is presented in Table 1 for all human dried skulls. Figure 1 shows the photograph of bilateral CCL and CCF and Fig 2 shows photograph of unilateral (right side) complete CCF and ossified CCL. It is observed in the same photograph that left side CCF is absent, mere space is seen and CCL is partially ossified Figure 1: Bilateral CCL and CCF Figure 2: Right side CCL and CCF
DISCUSSION The anterior clinoid process forms the attachment site for the free anterior margin of the tentorium cerebelli, whereas the middle clinoid process provides the attachment for diaphragm sellae (Grays’ anatomy). The parts of the sphenoid bone that are usually reported as capable of ossification are the pterygospinous and interclinoid processes. The anterior clinoid process may be joined to the middle clinoid process by a ligament or dural fold. When ossification of the fibrous ligament connecting the anterior clinoid process to middle clinoid process occurs, the carotico clinoid foramen is formed. In absence of ossification of fibrous ligament, mere space is seen between anterior and middle clinoid process. The ossification of a fibrous ligament is considered a normal physiological process that occurs with age6. Moreover the study byHochstetter andKier EL9,11 revealed the presence of this foramen in foetuses and children. The incidence of the presence of caroticoclinoid foramen was significantly lower in the study of Friere et al7 i.e. 8.5% of cases showed carotico clinoid foramen, while in the study of Erturk et al6 it was 35.67%. In the present study it was observed as 28%. According to the side, this study resulted in the incidence of more number of carotico clinoid foramen on right side than left. (Right = 21 Left = 19) In the other studies Ozdogmus et al14 studied 50 human skulls in Turkish population, incidence of carotico clinoid foramen on right side was 26 and left was 29. Gupta et al8 observed 14 caritico clinoid foramen out of total 70 skulls. Friere et al7 observed 7 on right and 2 on left side. When the foramen is analysed for diameter, sexual variation is found but it is not statistically significant. Friere et al7 studied the mean diameter regardless of sexes. They observed that on right side diameterwas 0.51cm and left was 0.53cm. In the present study the mean diameter in males on right side is 0.56cm on left side is 0.55 whereas in females mean diameter on right side is 0.54 and on left is 0.53cm. In the present study antero posterior length of this foramen is measured and mean of thisantero posterior length in males on right side is 0.79cmand on left side is 0.64cm while infemales, on right side is 0.77cm and on left side is 0.60cm. The present study, Friere et al7 and Erturk et al6 performed the measurements of carotico clinoid foramen in order to report that presence of this foramen may cause compression of the internal carotid artery. Therefore, if the calibre of internal carotid artery is more than the diameter of carotico clinoid foramen, there is high possibility to induce a headache caused by compression internal carotid artery in the presence of this foramen. This feature is important for the choice of surgical removal of anterior clinoid process14. Changes in internal carotid artery may cause compression of the cavernous sinus due to its medial position8,13. Das et al3-4 showed that presence of carotico clinoid foramen causes morphological changes in the internal carotid artery in almost all cases. The internal carotid artery is conventionally divided into six segments and the clinoid segment of the artery is located between the proximal and distal rings1. In any surgery involving exposure of the clinoid segment of the internal carotid artery excision of anterior clinoid process is mandatory. Even to expose the cavernous sinus and to manage paraclinoid aneurysm, the anterior clinoid process has to be removed5. The clustering of the neurovascular structures in the vicinity of the anterior clinoid process renders the surgery more risky. Sekhar and Akh15 showed the position of carotico clionoid foramen in an area close to the cavernous sinus. The formation of the carotico clionoid foramen may change the dimensions of this area. In conclusion if an ossified carotico clinoid ligament is present, it is likely to cause compression of the internal carotid artery. Anatomical knowledge of the dimensions of the carotico clinoid foramen may be useful in cases of surgery involving removal of anterior clinoid process.
CONCLUSION Presence of CCF is likely to cause compression of internal carotid artery and position of CCF close to cavernous sinus may change dimensions of this area and also cause morphological changes in internal carotid arteryin almost all cases. Morphometry of CCF may be useful in removal of anterior clinoid process (ACP) for which additional risk is involved.
REFERENCE
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.