 Home
Home|
Table of Content Volume 8 Issue 2 - November 2018
Growth pattern of genu varum and valgum in Indian tribal children of Jharkhand state
Dhananjay Kumar1, Shanmukha Varalakshmi Vangara2*, Patnaik V V Gopichand3, Nidhi Puri4
1,2Assistant Professor, Shri Ram Murthi Smarak Institute of Medical Sciences, Bhojipura, Bareilly, U.P, INDIA. 3Professor and Dean, Mamata Medical College and Hospital, Hyderabad, Telangana, INDIA. 4Professor, Dr Yashwant Singh Parmar Government Medical College Nahan, Himachal Pradesh, INDIA. Email: lakshmidhananjay@gmail.com
Abstract Background: Genu varum- valgum can be determined by measuring tibiofemoral angle (TFA), intercondylar distance (ICD) and intermalleolar distance (IMD). Current study establishes the reference values of TFA (degrees) in normal healthy tribal population of Ranchi district. Previous studies have noted the regional differences in TFA. Despite its clinical importance and social relevance, literature is scanty in Indian population especially in northern India tribal children. Material and Methods: A cross sectional study is performed to assess the knee angle. 360 tribal children aged between 2-14 years were recruited in this study. TFA of children was measured using clinical methods with the help of universal goniometer. Anthropometric variables like height, weight and body mass index (BMI) were noted for all subjects to establish their relationship with TFA. Results: Mean TFA was 4.84°±2.39° (Min=-0.75°, Max 12°) with range (4.59° to 5.08°). The knee angle at the age of 2 years was 1.21° mean valgus with range 0.82° to 1.59°, min -0.75° and max 2.25°, thereafter a progressive increase, with peak mean valgus of 6.63° ranging 5.91° to 7.34° at 7-8 years of age was noted. Later, there was notable decrease in TFA, which ultimately stabilized to a mean value of around 5°. Maximum mean valgus was 12° at 7-8 years of age group. Conclusion: This study provides age wise baseline data and range of physiological TFA. This data of 2 to <14 years age group tribal children of JH is helpful to the orthopaedic surgeons, physicians, paediatricians, radiologists, and physiotherapists for reconstruction and management of genu varus and valgus deformities. Key Word: Genu varus, Genu valgus, Anterior superior iliac spine (ASIS), Intermalleolar Point, Tribal Children.
INTRODUCTION The mid longitudinal axes between femur and tibia form an angle, which changes from birth to age of 9-10 years. The angulation between femur and tibia presents genu varum at birth, which changes to genu valgum as the children starts to walk. Genu varum (GVR) is also termed as ‘bowleg’. It is an outward curvature of both femur and tibia, marked by medial angulation of the leg in relation to the thigh. Genu valgum (GVL), commonly called as ‘knock-knees’ is a condition where both knees touch one another when the legs are straight. Genu varum -valgum is a relatively common finding in children among all angular deformities of lower limb. Mild to moderate bowlegs in newborn and knock- knees in early childhood are well-defined common orthopedic problems. Both pediatricians and pediatric orthopaedic surgeons are frequently encountering these situations. Mostly it is benign and self-limiting, although these deformities cause a great concern to the parents and relatives, such apprehension among parents forces the physicians to conduct physical or radiological examinations. The amount of varosity and valgosity is age specific, gender specific and racial specific.3 It also depends on daily habits of the child. Genu varus and valgus are measured either in terms of tibiofemoral angle (TFA) in degrees or intercondylar distance (ICD) and in intermalleolar distance (IMD) in centimetres. Knowledge of normal limits of the TFA in specific population is important for explanation of informative details to parents. Radiologic, photographic, and clinical techniques have been used to assess the normal limits in TFA. Current study establishes the reference values of TFA (degrees) in normal healthy tribal population in Ranchi district of Jharkhand (JH) state. A tribe is a group of individuals with common verbal communication, parlance, territory and monetary system. They have unique oral traditions and customs of antiquity that is entirely different from civilized societies. There are 32 identified tribal groups in JH as per the constitutional criteria of Scheduled Tribal act. Tribal people of JH belong to Proto-Australoid race. Baraik, Bedia, Bhagat, Gudia, Hembrom, Kachhap, Khelko, Kujur, Lohra, Munda, Mahli, Oraon, Pahan, Sinku, Tirkey, Toppo are the main tribal groups of Ranchi district. Their physical features represent short stature, long cephalus, broad flat nose and dark skin. They mostly reside in villages, consists of many tolas. Houses are mostly made of mud with thatched roofs. Their staple food is rice, fruits, flesh of animals and birds. Beer prepared from rice called Haria is their favourite drink. Physical and socio-cultural aspects of tribals have great importance as they are the true representatives of our past sequence of development. They can be considered as ‘living history or living fossils’ of our early stages of development. Despite its clinical importance and social relevance, literature is scanty in Indian population especially in north Indian tribal children.
MATERIALS AND METHODS Sample size of total 360 children of Jharkhand (JH) was participated in current study with 180 girls and 180 boys from 2 to 14 years age groups. Subjects were classified into twelve specific age groups. Each age group comprised 30 children with15 girls and 15 boys. They were randomly selected from different Aanganwadi, Primary and Middle schools. In case of younger children, age was verified by documents from the schools or immunization cards. In case of lack of proper documentation, regional festivals or lunar aspects described by parents regarding date of birth were taken into consideration. Exclusion criteria: Children <2 years (years) and >14 years, Other than tribals of JH states, Musculoskeletal system disorders (developmental dislocation of hip, skeletal dysplasia, cerebral palsy, neuromuscular disorders, foot deformities, leg length discrepancy of >2cm), Surgery of lower limb, Parents who did not give written consents were also excluded.
Measurements: Approval by the Institutional ethical committee was obtained in priori. The letter was presented to the school head/principal of each school visited. The methodology, aims and objectives of the study were explained to Head Teacher/Principal in simple terms. Skin marker was used to mark dots over the ASIS, centre of patella and the intermalleolar point (midpoint between the tibial and fibular malleoli). Then two longitudinal lines were drawn using the marker and the ruler; one connecting ASIS and the centre of patella (femoral axis) and the other connecting the center of patella and the Intermalleolar point (tibial axis). TFA was measured with help of goniometer. The fulcrum of goniometer was placed on the centre of patella; the stationary arm was on femoral longitudinal axis and the movable arm on tibial longitudinal axis. The angle between them was measured (Figure-1). TFA was assessed as neutral, varus and valgus knee when values were zero, negative and positive respectively. Height and weight were measured with subject in light clothes and barefooted, using standard apparatus. Weight was measured to the nearest 0.5 kilogram (kg) using a weighing scale which was set to zero reading before each measurement. Height was measured to the nearest 0.1 centimetres (cm) using a measuring tape.
Figure 1: Goniometric measurement of TFA
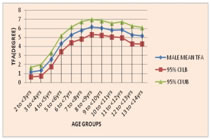
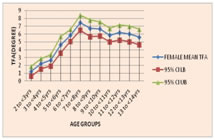
RESULTS The knee angle at the age of 2 years was mean valgus of 1.17° and 1.25° in male and female children respectively. Thereafter, a progressive increase with peak mean valgus of 6.17° at 8 to < 9 years of age in males and 7.47° in females was noted at 7 to < 8 years of age. Later it decreased and ultimately stabilized to a mean around 5° in male and 6° in female. Overall mean was 4.57° and 5.10° in males and females respectively. Maximum mean valgus was 9.50° at 6 to < 7 years in males and 12° at 7 to < 8 years of age group in females (Table-1, Figure-2and3). There were significant gender differences at 3 to < 4, 7 to < 8 years age group and in overall study population at p= 0.022. Girls had higher valgus than boys in each age group, but results were not statistically significant (Table-1, Figure-4). Significant gender differences were noted between BMI and TFA at p<0.05(Table-2). TFA established significant positive correlation between age, height, weight and BMI at p = 0.001 (Table-3).
Table1: Independent t- test between Male and Female TFA
TFA-Tibio femoral angle; years- Years; SD- Standard Deviation; CI- Confidence Interval; LB- Lower Bound; UB-Upper Bound; t- Independent t-test value; p- probability
Figure 2: Baseline data of TFA in male children Figure 3: Baseline data of TFA in female children Figure 4: Comparative baseline data of TFA Table 2: Independent t- test of all Parameters
TFA- Tibio femoral angle; BMI- Body Mass Index; years- Years; SD- Standard Deviation; df- degree of freedom; t-Independent t-test value; p- probability
Table 3: Correlation of TFA with other parameters
TFA- Tibio femoral angle; BMI- Body Mass Index; Sig. - Significance DISCUSSION Somatometric parameters in terms of standing height, body weight were measured. BMI was calculated to understand growth patterns. Mean height and weight of male children was more than that of females. The sexual dimorphism observed in this study was in consonance with the previous study conducted by Vangara et al.3 There was significant gender differences in BMI and TFA at p<0.05. Physiological varus is a normal condition most commonly observed in children of <2years.3.5 In this study physiological varus beyond 2years of age was found to be minimal. It was seen up to 3 to <4years of age in female children while male children were noted to have varus till 4 to <5years. According to our previous study physiological varus in case of Andhra Pradesh tribal children was seen up to 3 to < 4years of age in females and 5 to < 6years in males.3The mean TFA at 2years of age group was positive, representing mean valgus alignment. This study found 2.8% and 2.2% GVR, 3.3% and 2.2% neutral in male and female children respectively. Our previous study reported 2% and 1% varus, 2% and 3% neutral in male and female children respectively.3 Current study is in agreement with previous Indian study conducted by Mathew et al. However they pointed out 2.7% of varus between 4-17years age and they considered it as pathological. This variation may be due to heterogeneous samples selected by them from a tertiary hospital. In the intrauterine life due to the constraint of space within the uterus, lower extremity is forced to lie in “Buddha” position with flexed hips and knees, internally rotated tibia and feet. It causes contracture of the medial knee capsule. In postnatal life during first year of age when children try to stand and walk, they rotate the tibia externally to put the foot straight ahead. Due to the external rotation of tibia, there is obligatory external rotation of femur. This position of femur makes the bowleg more exaggerated. The peak mean GVL of 6.17° was reached at 8 to <9years of age in males, while in females it was 7.47° observed at 7 to <8years (Table-1). Maximum mean knee valgus observed was of 7.6° in girls at 6-7years and 6.46° in boys at 7-8years and 6.6° at 7-8years in overall study population of Andhra Pradesh tribal children.3 Saini et al7 found mean peak knee valgus of 8°at approximately six years of age in mixed population of Indian children from a tertiary hospital. Cheng et al.7 also observed same peak mean valgus as Saini et al., but it was in early life at 3.5years age in Chinese children. Salenius et al.7 observed peak mean valgus of 12º at 3years in Finland children. Engel et al. found that knee angle reached to peak mean valgus of 6º-7º at 2-3years age, while Sabharwal et al. noted peak mean TFA of 9º valgus in American children of 6years age. Kaspiris et al.10 observed peak mean TFA around 7º at 3years of age using clinical methods in 3-9years age group normal South-West Greece children. Yoo et al.5 recorded peak mean valgus alignment of 7.8º at 4years in Korean children. Bafor et al10 found peak valgus of 7.87° TFA in 3years old Nigerian children of 3-10years age group. Arazi et al10 observed peak mean valgus of 9.8° and 9.6° at 6years in girls and 7years in boys respectively using the goniometric method in 3-17years age group Turkish children. In this study population, 93.9% and 95.6% were GVL in male and female children respectively. Our previous study in Andhra Pradesh tribal children found 96% and 97% valgus in male and female children respectively.3 These results were in consonance with the fact that peak mean valgus was observed prior in females than in males. It was also observed that female attains peak valgus one year earlier than male children do. As children start to walk, they like to hold their feet wide apart to increase stability, which exerts pressure on the lateral side of knees. It results in medial part of the epiphyseal plate to grow faster, causing laxity in medial ligament of knee and thus the amount of valgus increases. Due to this medio-dorsal beaking in metaphysis of proximal tibia and distal femur, thickening in cortex, reduction in size of epiphysis of distal femur occurs. Maximum valgus angle of 12° was noted at 7 to <8years of age group children. In this age group 9.50° and 12° TFA was found in male and female children respectively. As reported previously, valgus angle of up to 12° to 14° might be normal for the age groups of 6–7years and 7-8years in male and female respectively of Andhra Pradesh tribal children and needs only observation. 3 Heath et al.2 found maximum valgus of 8.7º at the age of 4years. Mohd-Karim et al.6 measured TFA clinically on normal healthy Malaysian children and observed maximum valgus angle at 3years of age. The maximum mean TFA noted by them for boys, girls and all children were 8.91°, 8.56° and 8.73° respectively. Saini et al.8 noted maximum valgus angle of 11° in 5-6years age group children in India. Reports of this study were in concordance with that of Saini et al. who observed a maximum valgus angle of 11° during 5-6years. Maximum valgus angle noted was more in comparison to all other previous studies mentioned. The varus - valgus alignment depends on growth of its articular cartilages and growth plates in the adjacent femur and tibia. The plates typically grow faster than the articular cartilages. Varus develops if the lateral side of plates grow faster than the plate of medial side. Variation in bone morphology from region to region specifically at proximal tibia, distal femur, patellar grooves are the reasons for these racial variation. After attaining peak valgus, TFA decreased continuously beyond 8 to <9years to a mean value of 5.18° in males and 5.63° in females. After 7 to <8years it reached up to 5.63° in female and 5.18° in male children. Yoo et al.5 recorded the same pattern of adult valgus in children older than 4 years. TFA decreased slowly to 5º-6º at 7-8years of the age in Korean children. Saini et al8 observed that beyond 6years of age, the valgus angle decreased and stabilised around 4°-5° in most children after the age of 10years. Salenius et al.10 observed constant mean valgus of 5º-6º between 7 and 12years in 0-16years age group of Finland children. Engel et al11 found that knee angle in American children remained as constant valgus of 4º-5º between 5-12years of age. Kaspiris et al.13 in 3-9years age group normal children of South-West Greece found that the TFA was around 4 º at the age of 7-8years. Sabharwal et al.12 noted constant 5º-7º valgus from the age of 7-18years in American children. Oginni et al.6 observed TFA of 6° from 4-12years of age. Cheng et al.9 found that in Chinese children greater than 3.5years age group, valgus angle gradually decreased up to1º by 8.5years age. Cahuzac et al.16 studied TFA in European children of 10-16years age group. They observed stable valgus angle of 5.61º to 5.53º in 10-16years female children. In boys, the valgus gradually decreased to a mean of 4.4º TFA. Omololu et al.18 noted that valgus angle remained constant throughout 1-10years of age with a mean angle of 11º. Akinpelu et al.18 studied knee angle in 1-10years age group Nigerian children. They found that valgus angle steeply decreased after 3 years till the 6years of age from 14.7º-9.6º. Later it was stabilised with increment to10.3°at 10years of age. Fakoor et al17 carried out cross-sectional study in Ahwaz, Iran, on 3-16years age group and observed that TFA after 3years decreased continuously up to 4.7° and 4.22° in males and females respectively up to 16years of age group. This study showed greater knee angle during stabilization when compared to other Indian studies. Tribials are the true representatives of our past sequence of development because of their physical and socio-cultural activities. Their muscle strength may be a cause for this variation. Higher degree of adult valgus is better than lesser degree of adult valgus because the chance of shifts from adult valgus angle to pathological varus is common in old age. This is due to the overweight and adoption of static lifestyle like pooja and namaz for a longer duration. TFA established weak and positive correlation between age, height, weight and BMI at p < 0.001. Current study is in well agreement with Fakoor et al.20 who found positive correlation of TFA with age (r=0.845), weight (r=0.55), height (r=0.769). Cahuzac et al.17 found no correlation between TFA and height(r= 0.031), weight (r= 0.064). Bafor et al.14 found significant negative correlation between the TFA and BMI as well as with weight. Arazi et al.15 also reported negative correlation between TFA and standing height as well as for weight in both boys and girls at p < 0.000. Mathew et al.7 found significant negative correlation between TFA and age, standing height at p< 0.001 after 5years of age.
CONCLUSION We have also provided 95% confidence interval of the mean TFA for each age group. These values can be used as a range of reference for Indian tribal children in future follow up studies. Children after 3years with varus alignment of the knee may be atypical and requires radiological evaluation, regular follow-up and proper management. We conclude that a valgus angle of up to 12° and 14° might be normal in Indian children in the age group of 6 to <7years and 7 to <8years in males and females respectively and needs only observation. 2years of age onwards till 6 to <7years should be considered as transitory period because there will be significant variation in valgus angle in this phase. It also indicates the stabilization of knee angle after 6 to <7years of age. Data also suggests that 7 to <11years is a safe period where no much variation in TFA can be noted. By 11 to <14years age variations in TFA between races and gender are noted. Children of 2 to <7years and 11 to <14years age groups are under transitory period and must be taken care of.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.