|
Table of Content Volume 8 Issue 3 - December 2018
A cadaveric study of level of carotid bifurcation and its variations
S H Dakare1*, P S Bhuiyan2
1Sr. Registrar, Department of Anatomy, HBTMC and Cooper Hospital, Mumbai-400056, Maharashtra, INDIA.
2Professor and HOD, Department of Anatomy, Seth G. S. Medical College, Parel, Mumbai-400012, Maharashtra, INDIA.
Email: sarika.dakare@gmail.com, drprithabhuiyan@gmail.com
Abstract Background: The common carotid artery normally bifurcates at the level of the upper border of the thyroid cartilage of the larynx (C3–C4 junction) into external and internal carotid arteries. There may be variations in the level of bifurcation. Aim: The aim of the study was to correlate level of carotid bifurcation with upper border of thyroid cartilage and observe variations in the level of bifurcation. Methods: Twenty formalin fixed adult human cadavers, obtained from the Department of Anatomy were dissected. Results: The common carotid artery bifurcation was found most commonly below the level of bifurcation in 41.03%, at and above bifurcation in 38.46%, 20.51% respectively. Conclusion: To know about the variations of carotid bifurcation is useful for surgeons performing head and neck surgeries. It is also helpful for radiologists for diagnostic imaging of vascular lesions and for interventional procedures.
Key Words: Bifurcation, Cadaver, Variations.
INTRODUCTION
The common carotid arteries differ on the right and left sides with respect to their origins. On the right, the common carotid arises from the brachiocephalic artery as it passes behind the sternoclavicular joint and on the left; it comes directly from the arch of the aorta in the superior mediastinum. Following a similar course on both sides, the common carotid artery ascends, diverging laterally from behind the sternoclavicular joint to the level of the upper border of the thyroid cartilage of the larynx (C3–C4 junction), where it divides into external and internal carotid arteries. Division of the common carotid may occur higher, near the level of the hyoid bone, or, more rarely, at a lower level alongside the larynx1. The knowledge about these variations is important for vascular surgeons as well as radiologists.
MATERIAL AND METHODS
Twenty formalin fixed adult human cadavers of undetermined age and gender (forty sides of neck) were dissected for this study. One specimen was excluded as it was having carotid tumor. Exclusion criteria for this study were cadavers with any traumatic lesions on neck, evidence of any surgical procedure on neck and any tumour in neck region. This study was done with due permission of Institutional Ethics Committee. Level of carotid bifurcation was observed in correlation with upper border of thyroid cartilage. Descriptive statistical methods are used for analysing data.

Figure 1: Illustration showing determination of level of carotid bifurcation
(ECA–External Carotid Artery, ICA-Internal Carotid Artery, CCA-Common Carotid Artery)
OBSERVATIONS AND RESULTS
In this study, the level of carotid bifurcation was observed and it was correlated with upper border of thyroid cartilage. Then the specimens were classified into 3 divisions as high level of bifurcation (those above upper border of thyroid cartilage), low level of bifurcation (those below upper border of thyroid cartilage) and normal level of bifurcation (at the level of upper border of thyroid cartilage). In this study, eight specimens were observed with high level of bifurcation of common carotid artery and sixteen specimens were observed with low level of bifurcation of common carotid artery. The percentage of specimens under each of this division is mentioned in the below table.
Table 1: Percentage of different levels of bifurcation of common carotid artery in relation with upper border of thyroid cartilage:
Level of Bifurcation of Common Carotid Artery |
Right (n=19) |
Left (n=20) |
Total (n=39) |
(%) |
Normal (At upper border of thyroid cartilage) |
07 |
08 |
15 |
38.46 |
High (Above the upper border of thyroid cartilage) |
06 |
02 |
08 |
20.51 |
Low (Below the upper border of thyroid cartilage) |
06 |
10 |
16 |
41.03 |
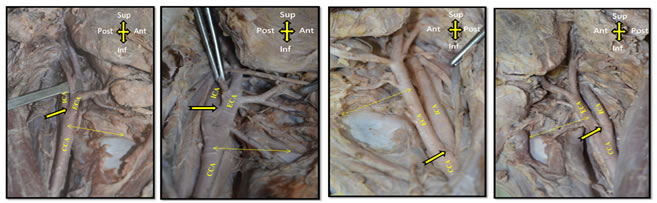
Figure 2 Figure 3 Figure 4 Figure 5
Figure 2 and 3: Illustrations showing high bifurcation of common carotid artery (ECA–External Carotid Artery, ICA-Internal Carotid Artery, CCA-Common Carotid Artery and Bold yellow arrow-level of bifurcation)
Figure 4 and 5: : Illustrations showing low bifurcation of common carotid artery (ECA–External Carotid Artery, ICA-Internal Carotid Artery, CCA-Common Carotid Artery and Bold yellow arrow-level of bifurcation)
DISCUSSION
Carotid bifurcation is one of the common sites of atherosclerosis. Carotid stenosis due to atherosclerotic plaques can lead to cerebrovascular accidents3. Awareness about variations in the level of bifurcation helps to avoid complications during vascular surgeries carotid endarterectomy, extracranial / intracranial arterial bypass. Knowledge about these variations is also important during intraarterial administration of chemotherapeutic agents and carotid catheterization4.
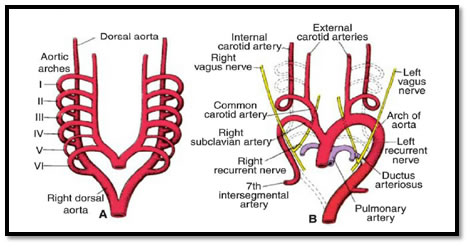
Figure 6: A. Aortic arches and dorsal aortae before transformation into the definitive vascular pattern; B. Aortic arches and dorsal aortae after the transformation. (Broken lines indicates obliterated components)
During development of aortic arch system, common carotid artery and the first part of the internal carotid artery are developed from third aortic arch and second aortic arch disappears. The external carotid artery is sprout of the third aortic arch2. In case of high carotid bifurcation, the internal carotid artery may develop from the second aortic arch and parts of the dorsal aorta above the level of the second aortic arch; instead of third aortic arch4. Normally, the dorsal aorta between the entrance of third and fourth arches, known as ductus caroticus is obliterated. If there is persistence of ductus caroticus then it may lead to low bifurcation of common carotid artery5. The following graph shows comparison of percentage of different levels of bifurcation from previous studies; with that of the present study.
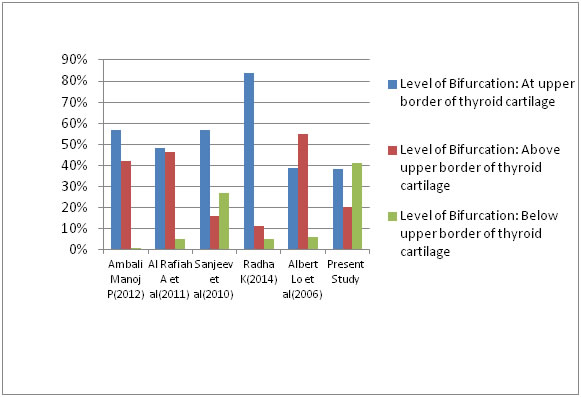
Figure 7: Comparison of level of bifurcation of common carotid artery in various studies
CONCLUSION
The different variations observed during this study will be useful for vascular surgeons performing head and neck surgeries. It will also help radiologists for diagnostic imaging of vascular lesions and for interventional procedures.
REFERENCES
-
Standring S. Gray’s Anatomy: Anatomical Basis of Clinical Practice. 40th ed. Edinburgh: Elsevier Churchill Livingstone, 2008
-
Sadler T W. Langman’s Medical Embryology. Thirteenth edition. China: Wolters Kluwer, 2015
-
Acar M, Salbacak A; Sakarya M E, Zararsiz I and Ulusoy M. The morphometrical analysis of the external carotid artery and its branches with multidetector computerized tomography angiography technique. Int. J. Morphol 2013; 31(4):1407-1414
-
Gluncic V, Petanjek Z, Marusic A, Gluncic I. High Bifurcation of Common Carotid Artery, Anomalous Origin of Ascending Pharyngeal Artery and Anomalous Branching Pattern of External Carotid Artery. Surg Radio Anat 2000; 23:123-125
-
Gailloud P, Murphy K J, Rigamonti D. Bilateral Thoracic Bifurcation of the Common Carotid Artery Associated with Klippel-Feil Anomaly. AJNR Am J Neuroradiol 2000; Vol 21:941–944
-
Ambali M, Jadhav S. Variations in Bifurcation Point and Branching Pattern of Common Carotid Arteries: A Cadaveric Study. J Pharma Biomed Sci 2012; 25(25):147-151
-
Al-Rafiah A, EL Haggagy A, Aal I, Zaki A. Anatomical Study of Carotid Bifurcation and Origin Variations of the Ascending Pharyngeal and Superior Thyroid Arteries. Folia Morphol 2011; 70(1):47-55
-
Radha K. Bifurcation Level of the Common Carotid Arteries: A Cadaveric Study in South Indian Population. Int J Anat Res 2014; Vol2 (3):511-514
-
Albert Lo Et al. Anatomical Variations of the Common Carotid Artery bifurcation. ANZ J Surg 2006; 76: 970–972
-
Iimura A et al. Anomalous Bifurcation and Island Formation of the Carotid Artery. Okajimas Folia Anat Jpn 2010; 86(4):121-128
-
Snjeev I K, Anita H, Ashwini M, Mahesh U, Rairam G B. Branching Pattern of External Carotid Artery in Human Cadavers. Journal of Clinical and Diagnostic Research 2010;15(4): 3128-3133
-
Hayashi N Et al. Surgical Anatomy of Cervical Carotid Artery for Carotid Endarterectomy. Neurol Med Chir (Tokyo) 2005; 45:25-30
-
Ito H, Mataga I, Kageyama I, Kobayashi K. Clinical Anatomy in the Neck Region- The Position of External and Internal Carotid Arteries May be Reversed. Okajimas Folio Anat Jpn 2006; 82(4):157-168
-
Thwin S, Soe M, Myint M, Than M, Lwin S. Variation of The Origin and Branches of the External Carotid Artery in Human Cadaver. Singapur Med J 2010; 51(2): 40
-
Heltzel S, Jelinek L, Jaynes D. Variation in the Caudal Branches of the External Carotid Artery: Comparison of Sex and Side. Medical Research Archives 2015; Issue 1:1-10
-
Chitra R. Trifurcation of the right common carotid artery. Indian J Plast Surg. 2008 Jan-Jun; 41(1): 85–88
-
Anangwe D, Saidi H, Ogeng’o J, Awori K O. Anatomical Variations of the Carotid Arteries in Adult Kenyans. East African Medical Journal May 2008; Vol. 85(5)
-
Anu V R Et al. Clinically Relevant Variations of the Carotid Arterial System. Singapore Med J 2007; 48(6): 566-569.
|
|
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.