 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 3 - June 2019
Role of serum vitamin D and calcium in chronic otolaryngological diseases
Arati Ganiger1, K Mallikarjuna Swamy2*, Amareshwara M Maligi3
{1Assistant Professor, 3Professor & HOD, Department of Biochemistry} {2Associate Professor, Department of ENT} KIMS, Koppal, INDIA. Email: coolarati123@gmail.com
Abstract Background: Vitamin D also known as sunshine vitamin, a fat-soluble vitamin having diverse biological effects. The purpose of this study is to put some light on the relationship between serum calcium, Vitamin D and ENT disorders. Objectives: To estimate serum 25-hydroxy vitamin D(25-OH Vitamin D) and serum calcium levels in ear , nose and throat cases not responding to conventional medical treatment. Materials and methods: It is a observational study. The study was conducted on 100 patients attending outpatient department (OPD) of otolaryngology clinic with various otolaryngological diseases such as chronic pharyngitis, chronic Suppurative Otitis Media(CSOM), cholesteatoma and upper respiratory tract infections (URTI) who were not responding to conventional medical treatment. These patients were advised for assessment of serum vitamin D [25 (OH) D] level and calcium levels to study the relationship between calcium and vitamin D and the otolaryngological diseases. Results: The serum vitamin D levels and serum calcium levels were found to be significantly decreased in cases. The results of vitamin D supplementation as well as calcium supplementation were promising in cases of pharyngitis, URTI with asthma, CSOM. Conclusion: Correcting vitamin D deficiency and calcium levels help in fast recovery of unresponsive cases. Key Word: chronic otolaryngological diseases.
INTRODUCTION Vitamin D, also known as sunshine vitamin is a fat soluble vitamin having diverse biological effects. It is synthesized from 7-dehydrocholesterol in the skin. The vitamin D binding protein transports the vitamin D3 to the liver where it undergoes hydroxylation by 25 hydroxylase enzyme to 25-hydroxy vitamin D (25 (OH) D) (the inactive form of vitamin D). Then further it is transported to the kidneys where it is hydroxylated by the enzyme 1 alpha hydroxylase to 1, 25 dihydroxy vitamin D [1, 25(OH) D], its active form. This enzyme is also present in a variety of extrarenal sites, including osteoclasts, skin, colon, brain, and macrophages, which may be the cause of its broad-ranging effects1.The role of vitamin D in prevention of respiratory tract infection, cochlear deafness or demineralization of bone is gathering evidence hence this study was conducted to evaluate the incidence of vitamin D deficiency in outdoor patients of otoryngology clinic with various symptoms and signs of E.N.T and related diseases . There is huge role of calcium in the maintenance of immunity in the body and it aids to fight off against the microbes from the environment. The purpose of this study is to put some light on the relationship between Calcium, Vitamin D and ENT disorders. The pleiotropic effects of this hormone outside the skeletal system have been recently studied. Vitamin D deficiency has been consistently associated with hypertension, diabetes mellitus, cardiovascular disease, stroke, multiple sclerosis, inflammatory bowel disease. The role of vitamin D in prevention of respiratory tract infection or aggravating demineralization of bone is gathering evidence and hence this study was conducted to evaluate the same in OPD cases of ENT. Many pathogens are sensitive to antimicrobials, cathelicidin and defensin released by the body under the influence of vitamin D2-5. The role of Vitamin D deficiency has also been attributed to cochlear deafness representing with trough shaped pure tone audiogram with a dip in 1 kHz and 2 kHz frequencies6
MATERIALS AND METHODS This was a observational study. The study was carried out on 100 cases attending the otorhinolaryngology(ENT) out patient department(OPD) of Koppal Institute of Medical Sciences(KIMS), Koppal, with various otolaryngological complaints and not responding to the conventional medical treatment. The study was carried out for a duration of 2 years. Such cases were advised for measuring serum levels of 25-OH Vitamin D and serum calcium levels. The age, sex, colour of skin, occupation, chief complaints, incidence of sun exposure was noted in all cases. Inclusion Criteria: The patients between 5 to 50 years of age of either sex attending outpatient of ENT with complaints of 1)Chronic Pharyngitis, 2) CSOM, 3)Cholesteatoma, 4) URTI. Vitamin D deficiency was defined as serum values < 20 ng/ml7 (Table 1) Exclusion criteria: Patients of diabetes mellitus, cardiovascular, hepatic or renal diseases were excluded from the study. Biochemical analysis: Venous blood sample of 3 ml was collected under aseptic precautions in a plain vial. It was allowed to clot and serum was separated by centrifugation.
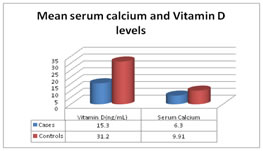
If electing to test vitamin D status, serum 25 hydroxy vitamin D(25-OH vitamin D) is the accepted biomarker.8 Although1, 25-OH-D is the active circulating form of vitamin D, measuring this level is not helpful because it is quickly and tightly regulated by the kidney. Statistical methodology: Data was expressed in terms of mean ± SD. Unpaired ‘t’-test was used to study the changes in serum vitamin D and calcium levels among cases. Pearson correlation was performed to establish the relationship between study variables. p value <0.05 was considered statistically significant. RESULTS This was a observational study conducted on 100 cases. The most common age group of cases was between 15-20 years. The mean serum 25-OH vitamin D and mean serum calcium levels are shown in Table 2. The mean serum 25-OH Vitamin D levels (ng/mL) in cases was 15.3 ±7.1 ng/mL as compared to the normal values of vitamin D > 30 ng/ml. The serum calcium levels were found to be decreased of average of 6.3 ±1.6 (Normal 9-11 mg /dl) (Figure 1).
Table 1: Grading of vitamin D defiency
Table 2: Mean serum 25-OH vitamin D and mean serum calcium levels
Figure 1: Mean serum levels of vitamin D and calcium in cases as compared to normal serum value
DISCUSSION Our study showed a significant decreased levels of vitamin D and calcium levels in chronic cases who did not respond to conventional medical treatment. The epithelium which faces the environment directly like the skin and the respiratory mucosa are protected by innate immunity.9 Vitamin D has a major role in it as Toll like Receptor and vitamin D receptor are present on the macrophages governing the innate immunity10-12. Vitamin D also regulates the level of the enzyme CYP27B1. All of this in turn leads to secretion of Cathelicidin, the major antimicrobial13. Active1, 25 dihydroxy vitamin D also acts as a chemo attractant for neutrophils and monocytes14. Therefore, its deficiency definitely causes decreased immunity and increased cases of upper respiratory tract infection15. The respiratory epithelium also converts inactive vitamin D to active 1, 25 (OH)D3 to increase the expression of vitamin D regulated genes16. It is the key immunomudoulator and its deficiency will increase the incidence of URTI leading to Otitis Media retraction pockets and cholesteatoma. here is presence of typical compensation in the body related to Vitamin D levels. When the body reserves of vitamin D are low, the calcium gets depleted too as vitamin D fails to reabsorb calcium from the kidney and intestine. The decreased calcium activates the osteoclasts and up regulates bone resorption from dense bones first and then other small bones. Low serum levels of vitamin D metabolites may lead to osteoclastic activity (Osteoporosis) that is mobilization of calcium from bones may also result in secondary hyperparathyroidism. Radiologically it cannot be detected until more than 35 % demineralization of bone has been done. Demineralization of cochlea has also been observed in temporal bone tomography. The calcium and phosphorus content of woven bone of the otic capsule are much higher than other bones and hence may be more affected by deficient vitamin D and calcium levels. Again deficiency of Vitamin D will enhance osteoclastic activity of cholesteatoma.17 Now it is well known that deficiency of vitamin D lowers the immunity and may precipitate the recurrent attacks of upper respiratory tract infection leading to eustachian tube dysfunction which may complicate as cholesteatoma. We have to work out the deficiency of vitamin D and blood level of calcium to prevent this drastic disorder (cholesteatoma).
CONCLUSION We can hypothesize that osteoclastic activity will be potentially aggravated in deficiency of vitamin D and calcium. By supplementing vitamin D and calcium in deficient individuals, helps in speedy recovery of the patients. Hence, early detection and treatment of the deficiency helps in faster recovery and better outcome.
ACKNOWLEDGEMENT I would like to thank my teachers, my family for their constant guidance and support throughout the study.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.