 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 2 - August 2019
Mid-gestational serum calcium and magnesium levels in women with pre-eclampsia: A nested case control study
Namrata Raul1*, Pramod Ingale2, Bina Dias3, Minal Pore4, Shubhangi Wankhade5
1Tutor, Department of Biochemistry, KJSMC, Sion Mumbai, Maharashtra, INDIA. 2Professor and HOD, 3Associate Professor, 4Specialty Medical Officer, Department of Biochemistry, LTMMC and GH, Sion Mumbai, Maharashtra, INDIA. Email: dr.namrata2@gmail.com
Abstract Background: Pre-eclampsia is one of the important complications of pregnancy with unclear etiology. Many theories suggest abnormal placental implantation and abnormal trophoblastic invasion as possible causes. Since calcium, magnesium, contributes significantly in the functioning of the vascular smooth muscles, they may have their role in pathogenesis of preeclampsia. Aims and Objectives: To study correlation between mid-gestational low serum calcium and magnesium levels and subsequent development of preeclampsia. Material and method: In a prospective and longitudinal study, 443 nulliparous women between 20-35 years of age were enrolled at 20-25 weeks of gestation and were followed up till delivery for pregnancy outcome. Serum Calcium and magnesium levels were done at enrollment. Mid-gestational calcium and magnesium levels of the women who subsequently developed pre-eclampsia were compared with age matched controls that had uneventful pregnancy. Results: Serum calcium levels of cases were significantly decreased compared to controls (P <0.0001). On the other hand, Serum magnesium exhibited slightly decreased in cases as compared to controls, though the difference was not statistically significant. Conclusion: Low levels of Calcium and Magnesium found in our study suggest their role in pathogenesis of pre-eclampsia. Calcium supplementation during early pregnancy may be helpful in prevention of pregnancy induced hypertension. Key Word: Eclampsia.
INTRODUCTION Pregnancy is a physiological state associated with substantial and on occasion, profound alterations in metabolic and biochemical processes. Preeclampsia is a pregnancy-specific multi-systemic disorder characterized by proteinuria and the onset of hypertension after 20 weeks of pregnancy. It is a rapidly progressive condition characterized by high blood pressure, thrombocytopenia, edema of the lower extremities and protein urea.1 Multiparous women have an incidence of 6-7% and it occurs more frequently in primiparous women.2 Regardless of parity, multiple gestations have an incidence of 30%.2 Preeclampsia is believed to be multifactorial in origin, with risk severity influenced by both maternal and fetal determinants.[3] Women with preeclampsia do not usually demonstrate frank hypertension until second half of pregnancy, but vaso-constrictive effects may be present earlier. Alterations in vascular reactivity may be detected as early as gestational week 20.4 It is a major condition responsible for maternal and perinatal morbidity and mortality worldwide. 5 Calcium is a intracellular second messenger involved in many processes such as signal transduction, neurotransmission, enzyme and hormone secretion, cell cycle regulation and programmed cell death. It is a crucial element for adequate fetal development and prenatal programming of future diseases.6. Calcium is actively transported across the placenta to reach about 25–30 mg of Calcium at term in the fetus. About 80% of the total fetal Calcium is accumulated during the last trimester of pregnancy.7 This Calcium transfer allows adequate fetal skeleton mineralization and various cellular functions. Magnesium regulates vascular tone and reactivity and help in maintenance of normal blood pressure by synthesizing vasodilators like prostacyclins and nitric oxide.8 Also magnesium act as a calcium channel blocker which intern may reduce the release of calcium and thus decrease vascular resistance. In addition, activation of the Na-K ATPase pump by magnesium, that controls the balance of these minerals contributing to the homeostasis of electrolytes in cells.9 Several evidences indicate that various micro and macro elements might play an important role in development of preeclampsia. Calcium, magnesium, sodium and potassium are important in the functioning of the vascular smooth muscles. Various studies have shown association between low levels of these elements and preeclampsia. Hence, the present study was designed to evaluate role of calcium and magnesium in the preeclampsia
AIM To evaluate low serum Calcium, Magnesium levels as risk factor for preeclampsia.
OBJECTIVE To study correlation between mid-gestational low serum calcium and magnesium levels and subsequent development of preeclampsia. MATERIAL AND METHOD In a prospective longitudinal study, 500 nulliparous women between 20-35 years of age without any pre-pregnancy medical diseases were enrolled at 20-25 weeks of gestation. Serum Calcium and magnesium levels of all the women were done at the time of enrollment. All the women were followed up till delivery for development of preeclampsia and pregnancy outcome. Diagnosis of preeclampsia10
Proteinuria
Out of total 443 subjects included in the study, 43 developed preeclampsia. 86 out of 278 subject with full term delivery without any complications were included in control group. Serum Calcium and Magnesium levels of cases and controls that were measured at 20-25 weeks were compared. OBSERVATIONS AND RESULTS Table 1: Pregnancy outcome of women included in study
Table 2: Distribution of pregnancy induced hypertension
5 out of 48 subjects with preeclampsia also had gestational diabetes mellitus, therefore excluded from study group. 43 subjects with severe preeclampsia and 86 subjects out of 278 subject with full term delivery without any complications were included in cases and control group respectively. Table 3: Distribution of Serum calcium and magnesium in controls and cases
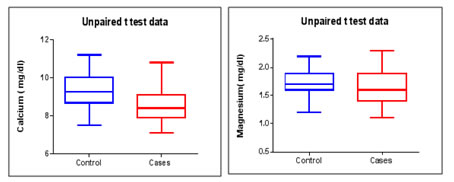
There was statistically significant decrease in calcium value of control as compared to cases (P<0.0001) Serum Magnesium levels of cases were low compared to control though the difference was not statistically significant. (0.052)
Graph 1 and 2: Distribution of Serum Calcium and Magnesium levels of controls and cases DISCUSSION Preeclampsia is one of the leading cause of maternal mortality and morbidity in India. Maternal death has grave effect on the surviving child.11 Incidence of preeclampsia in India is reported to be 8-10% of pregnancies in various studies, while it is four times higher in primipara than in multipara. Nulliparity is a strong risk factor, almost tripling the risk of preeclampsia (odds ratio of 2.91, 1.28 to 6.61) based on a systematic review of controlled studies. 12 In our study which included only primipara, 26.9% developed pregnancy induced hypertension and 9.8% showed signs of preeclampsia. In this study, we observed low levels of Calcium and Magnesium in preeclamptic women compared to women who had no complications during pregnancy. Serum calcium of cases were significantly decreased compared to controls.[Table 3, Graph: 1] On the other hand, Serum magnesium exhibited slightly decreased in cases as compared to controls, though the difference was not significant. [vide Table 3, Graph: 2] Similar results were seen in the study conducted by Jean-Daniel Lalau et al showed PIH having a negative correlation between blood pressure and plasma corrected calcium (r = -0.43, P < .05), which was in agreement with epidemiological studies of essential hypertension.13 An international study, in which calcium supplementation was given in women with low calcium intakes (<600 mg/dl) showed decrease in severity of the disease, however, did not find any reduction in incidence of preeclampsia.14. Low calcium intake results in high parathyroid hormone levels and increased membrane permeability, resulting in increased intracellular calcium levels and decreased serum calcium levels. The former triggers vascular smooth muscle contraction and contributes to increased blood pressure,15 release renin from the kidney, leading to vasoconstriction and retention of sodium and fluid. These changes may contribute to the development of PIH and preeclampsia.16 Increased renal clearance due to hemodilution during pregnancy and consumption of minerals by growing fetus leads to hypomagnesaemia.17 Magnesium levels have significant effects on cardiac excitability and on vascular tone, contractility and reactivity.18 Mac Donald et al have shown experimentally that magnesium has a role in vasoprotection. These findings support the fact that hypocalcemia and hypomagnesemia correlate to severe preeclampsia19 Lower levels of 1,25(OH)2D3 and PTH in hypertensive pregnancy have been seen in various studies and suggested that alterations in calcium regulatory hormones could contribute to the development of preeclampsia, and the symptom of hypocalcemia20. Other studies suggest that in preeclampsia the low levels of 1, 25(OH)2D3 cause a decrease in intestinal calcium absorption and serum ionized calcium. The lower ionized calcium causes an increase in PTH levels, which stimulate calcium loss from bones, and tubular reabsorption of calcium from kidney leading to hypocalciuria.21,22,23,24,25
CONCLUSION Intake of balanced diet fulfilling all nutrient requirement from pre-conceptional period is important for maternal and fetal wellbeing as well as for positive pregnancy outcome. Presence of low levels of these elements during early pregnancy suggest their possible role in etiology of preeclampsia. Supplementation of these elements in diet may be of value to prevent complications like preeclampsia during pregnancy.
LIMITATIONS We did not study Serum Calcium and Magnesium levels at the time of actual diagnosis of preeclampsia. Calcium and magnesium intake of the subjects was not assessed.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.