 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 3 Issue 1 - July 2017
Role of 25 hydroxy Vitamin-D in parkinson’s disease
Yogesh Krishna Sahay1*, Madhu Sinha2*
1Assistant. Professor, 2Associate Professor, Department of Biochemistry. Anugrah Narayan Magadh Medical College, Gaya, Bihar, INDIA. Email: dryogeshkrsahay@gmail.com
Abstract Problem statement: Parkinson disease is the second most prevalent neurodegenerative disease worldwide. In the initial stage of the disease, the most obvious symptoms are movement related, which include tremors, rigidity, slowness of movement and difficulty with walking and gait. Behavioural problems and dementia also appears in advanced stage of the disease. Depression is the most common psychiatric symptom and often associated with emotional disorder and sleep disturbances. The disease is common in older and mostly occur after 50 years of age. Methods: It was observational, and case control study to find out that vitamin-D could be regarded as a predictive bio-marker for severity of Parkinson’s Disease. A direct interview of the eligible study participants were carried out treatment sheets were reviewed and after duly explaining the procedures in their local languages. Detailed records of demographic and clinical features were noted in case record proforma. History of name, age sex, religion occupation symptom, duration, history of recurrence etc. was recorded. Patients with PD attended in the Medicine OPD were selected as cases. Total sample size was 30. All subjects was above the age of 60 years The period of the study was one (01) Year beginning from2015 to2016. Results: All cases and control are age match α = 30. Control groups were selected from the community. Fasting glucose level of control and case where within biological reference intervals, mean control value 88.22 ± 13.9 mean case 100.45 ± 8.79. The result is statistically significant p value- <001. Serum Calcium levels of both case and control group are within biological reference interval. Mean value in PD 8.45, SD ± 2.21 and for control 8.83 SD ± 0.49, p Value – <0.3999. It was statistically not significant. Serum level of Vitamin-D in Parkinson Disease (16.51 ± 3.08) is lower in comparison to control group (25.92 ± 3.96) p Value- 0.000. The result was statistically significant control group are within insufficiency range (20 – 29 ng/ml). Conclusion: All patients of our study showed a deficient level (less than 20 ng/ml) of vitamin-D. The control group surprisingly had vitamin-D level in insufficient range (20 – 29 ng/ml). The reason for this insufficient level of Vitamin-D may be searched for in future with large number of sample size. Key Words: Parkinson’s Disease, neurodegenerative Disease, Hypokinetic rigid syndrome.
INTRODUCTION Parkinson disease is a devastating neurodegenerative disorder characterized by progressive detritions of dopaminergic system in the substantia nigra, pars compacta. The prevalence of Parkinson disease is estimated to be 1 % to 5 % in individuals older than 50 years and rises steadily within a peak. Occurring between ages of 70 and 90 years. Parkinson disease is a disorder of CNS which affects movement; often including tremors. The disease is also known as Idiopathic or primary. Parkinsonsm, Hypokinetic rigid syndrome (HRS) or paralyses agitans is a degenerative disorder of CNS death of dopaminergic cells the substantial nigra and brain is considered as the cause of the disease. In this initial stage of the disease, the most obvious symptoms are movement related, which include tremors, rigidity, slowness of movement and difficulty with walking and gait. Behavioral problems and dementia also appears in advanced stage of the disease. Depression is the most common psychiatric symptom and often associated with emotional disorder and sleep disturbances. The disease is common in older and mostly occur after 50 years of age. “Parkinsonian Syndrome” is Idiopathic although some atypical cases have genetic cause. The incidence is less in tobacco smokers as during smoking dopamine and endorphin is released researches are going on for environmental positive agents like toxins which may trigger the disorder. Active metabolites of vit D 1.25 dihydroxy D is involved in calcium and phosphate metabolism and exerts a large number of biological effect. It down regulates parathormone secretion, active immunity and cell proliferation and also promotes insulin secretion, innate immunity and stimulate cellular differentiation role of vitamin D in immunoregulation has lead to the concept of dual function as both as important secosteroid hormones for regulation of body calcium homeostasis and as essential organic compounds that has been shown to have a crucial effect on the immunoresponse. Altered levels of vitamin D3 has been associated with a higher susceptibility of immune mediated disorder and inflammatory disease. Nearly 34.6 % of vitamin D deficiency subjects developed neurological disturbances.1Vitamin D belongs to the group of secosteroids compound, Vitamin D2 and D3 (D3 is mainly obtained through skin synthesis and D2 from mushrooms, yeast, plants etc. The dietary source of vitamin D is in fish, egg yolk, in the form of D3 in milk. Fortified food is another source for example milk, cereals in the form of vitamin D2.2,3 Vitamin D is biologically inert and is converted to active form by oxidative metabolic process. Vitamin D3 is primarily acquired endogenously by photochemical conversion of 7 dehydro cholesterol to pre-vitamin D3 in the skin with exposure to sunrays. Pre-vitamin D3 is converted to the inactive isomers tachysterol and lumisterol. This process is reversible as when pre-vitamin D3 level is low the process is reversed so that pre-vitamin D3 is converted vitamin D3 and enters metabolic pathways. The conversion takes place through thermic isomerization and transported to the liver bound mostly with vitamin D binding protein (DBP).4-7 Vitamin D acts through two types of receptors (1) The vitamin D receptor (VDR), a member of the steroid/ thyroid hormone super family of transcription factos, and (2) The MARRS (membranes associated rapid response steroid binding) receptor, also known as Erp57 / Grp58. In this article, we review some of the mechanism that may underlie the role of vitamin D in various brain diseases. Parkinson's disease (PD), a common disease of the elderly, is a movement disorder characterized by tremor, akinesia, and loss of postural reflexes, leading to immobility and frequent falls. It results from selective loss (death) of dopaminergic neurons in the substantia nigra region of the brain, largely developed prior to clinical diagnosis, and continuous after diagnosis, despite use of current therapeutic modalities. In PD in the United States the cause and mechanism of continued neuron cell death in the substantia nigra is currently unknown. We hypothesize, based upon several lines of evidence, that documented chronically inadequate vitamin D intake in the United States, particularly in the northern states and particularly in the elderly, is a significant factor in the pathogenesis of PD. This hypothesis implies that dietary aid for prevention and therapy for PD is possible.8,-10 Despite excessive hip fractures in patients with Parkinson's disease (PD), little is known about bone changes in these patients. Researchers measured bone mineral density (BMD; Z scores) in PD patients and analyzed its relation to serum biochemical indices and sunlight exposure. They also measured BMD in 71 patients in the second metacarpals and divided the patients into two groups according to functional independence: group 1, Hoehn and Yahr stages 1 and 2; and group 2, stages 3 to 5. In four of 20 patients in group 1 (20%), the Z scores was less than -1.0, indicating osteopenia. In 51 patients in group 2, 31 (61%) had a Z score less than -1.0. The group 1 patients showed a normal mean serum level of 25-hydroxyvitamin D (25-OHD; 21.7 ng/ml), while most group 2 patients were in a deficiency range (group mean 8.9 ng/ml). Many group 2 patients were sunlight deprived. Both groups had elevated serum ionized calcium levels correlating positively with Hoehn and Yahr stage and markedly depressed serum 1,25-dihydroxyvitamin D(1,25-[OH]2D) concentrations, indicating that immobilization-induced hypercalcemia had inhibited 1,25-[OH]2D production. Z scores correlated positively with 25-OHD levels and negatively with parathyroid hormone concentration and Hoehn and Yahr stage. Vitamin D deficiency due to sunlight deprivation and hypercalcemia induces compensatory hyperparathyroidism, which contributes to reduced BMD in PD patients, particularly those who are functionally dependent. Low BMD increases risk of hip fractures in patients with PD but may be improved by vitamin D supplementation.11
MATERIAL AND METHODS Type of study: Hospital based observational study. Study design: Case control study Study area: Department of Biochemistry and Medicine OPD in Anugrah Narayan Magadh Medical College, Gaya. Study duration: The period of the study was one (01) Year beginning from2015 to2016. Sample size: Patients with PD attended in the medicine OPD were selected as cases. Total sample size is 30. Study tools: A) Semi auto analyzer, B) Elisa Reader. Study technique: A direct interview of the eligible study participants were carried out treatment sheets were reviewed and after duly explaining the procedures in their local languages, informed consent was taken. Detailed records of demographic and clinical features were noted in case record proforma. History of name, age sex, religion occupation symptom, duration, history of recurrence etc. was recorded. Biochemical parameters: Blood glucose, Calcium, Vitamin- D. Collection of blood sample: Blood is collected from anterior cubital vein under aseptic condition. Fluoride vials were used for fasting blood sugar samples. Plain vials were used for calcium measurement. For estimation of vitamin D. Bloods samples of were properly covered with black paper to avoid exposure of sunlight.
RESULTS
Table: 1: Distribution of Glucose among case and control
Table No- 1. Shows that mean control value 88.22 and SD ± 13.9 mean case 100.45 and SD ± 8.79. The result is statistically significant p value- <.001
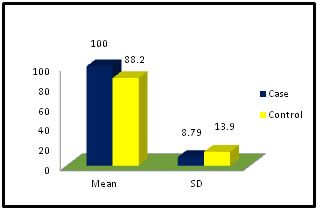 Figure 1: Distribution of blood glucose among case & Control Table 2: Distribution of Calcium among case and control
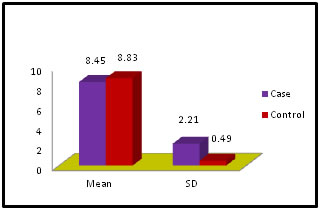
Table No-2. Shows that, the Serum Calcium levels of both case and control group are within biological reference interval. Mean value in PD 8.45, SD ± 2.21 and for control 8.83 SD ± 0.49, p Value – <0.399. Result is statistically not significant.
Figure 2: Distribution of Serum Calcium among case and control
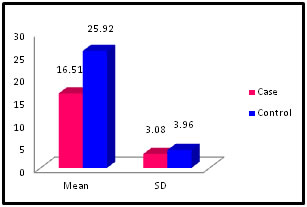
Table 3: Distribution of Vitamin-D among case and control
Table No-3. Serum level of Vitamin-D in Parkinson Disease (16.51 ± 3.08) is lower in comparison to control group (25.92 ± 3.96) p Value- 0.000. The result is statistically significant control group are within insufficiency range (20 – 29 ng/ml). PD subjects are within deficiency range (< 20 ng/ml).
Figure 3: Distribution of Vitamin-D among case and control DISCUSSION It was a hospital based case control study; we selected a total number of 30 subjects as cases with Parkinson Disease. All the subjects were above the age of 60 years. The patients were included for the study did not have other diseases like liver Cirrhosis and other chronic and infectious diseases. Controls were selected from the community population without suffering from PD and others systemic diseases. Our finding shows that out of 30, 4 numbers of female subjects are suffering from PD which constitutes 12.5% of the total study population. Routine FBS estimation was performed in both control and test group and the distribution between case and control reveals that for test case the mean FBS value is 100.45 with a standard deviation of± 8.79 and the FBS value for the control was 88.22 with a SD ± 13.9. This shows a little increase in FBS concentration in subjects of Parkinson’s Disease. According to the recommendation of American Diabetic association (2009), the biological reference interval of FBS concentration should be within 99 mg/dl. For glucose the result is statistically significant. Vitamin-D is responsible for normal homeostasis of calcium in the body, with this idea we included estimation of serum Calcium among the controls and cases of our study. Serum Calcium level in PD patients was found to be low normal as per the method we adopted. The biological reference interval is (8.4 – 10.2 mg/dl) Mean value of serum calcium of PD subjects were 8.45 and with a SD ± 2.21 and the mean value for control was 8.83 with a SD±0.49. This is not statistically significant p Value- 0.399. We performed a total 25 hydroxy vitamin-D estimation in both test and control groups and surprisingly all the control subjects had insufficient level of the vitamin( 20-29 ng/ml ). The mean value for control was 25.92 with a SD of ±3.96. Below 20 ng/ml indicates a deficiency of the hormone. The total 25 hydroxy vitamin-D concentration in patients of Parkinson’s Disease was in deficient range as revealed in this study. The mean value (16.51) with SD ± 3.08 and the p Value is 0.000. The result is statistically significant.
CONCLUSION The present study was conducted with an object to explore the association of neuro degenerative disorder and vitamin-D in patients attending Anugrah Narayan Magadh Medical College, Gaya, which was a tertiary care hospital, in collaboration with the department of medicine. Patients were attending this institution. Only a few published data and reports on our topic are available till date and so, we undertook the study. Patients over 60 of age and suffering from Parkinson’s Disease were selected as study groups. Control groups were selected from the community and all of them were above 60 years. All patients of our study showed a deficient level (less than 20 ng/ml) of vitamin-D. The control group surprisingly had vitamin-D level in insufficient range (20 – 29 ng/ml). The reason for this insufficient level of Vitamin-D may be searched for in future with large number of sample size. As our sample size is small it would be rational to conduct the study with large number of patients of Parkinson’s Disease which may indicate the necessity of estimation of vitamin-D in the disease and the deficiency when present, may be corrected by supplementation of Vitamin-D.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.