 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 1 - January 2018
Study of electrolyte imbalance in AMI
A M Siddiqui1, Sujata M Gaikwad2*, A R Shinde3
1Associate Professor, 2Jr. Resident, 3Assistant Lecturer, Department of Biochemistry, Dr. S. C. GMC, Nanded, Maharashtra, INDIA. Email: sujatagaikwadpbn@gmail.com
Abstract Background: Cardiovascular disease is one of the leading causes of morbidity and mortality across the world. Worldwide there are 3 million sudden cardiac deaths per year due to acute myocardial infarction. Different electrolytes such as calcium, potassium and sodium play an important role in the cell metabolism, electrical conduction and membrane excitability. Serum electrolyte imbalance after an episode of acute myocardial infarction is common. Abnormalities of these electrolytes due to different causes can lead to a significant cardiac life threatening events. Objectives: Study aimed to compare the prevalence and pattern of electrolye imbalance in both cases and controls. Material and Methods: This is a prospective study carried out on 90 subjects. Out of these 45 were clinically diagnosed cases of acute myocardial infarction and 45 were age and sex matched healthy controls. Blood samples were collected from all participants and analyzed for Serum sodium, potassium and calcium. RESULTS: In AMI patients serum potassium, calcium levels are significantly low while serum sodium level is low but showed no significant difference among cases and controls. Conclusion: Electrolyte imbalance maximally seen in Calcium. Hypocalcaemia was present in around half of total cases. Hypokalaemia was evident in a large number of patients in the early phase of AMI. Therefore it is recommended that calcium and potassium levels which affect the patients of acute myocardial infarction should be monitored, and potassium replaced whenever required. Key Words: Electrolyte imbalance, myocardial infarction, hypocalcaemia, hypokalaemia, hyponatraemia.
Cardiovascular disease is one of the leading causes of morbidity and mortality across the world. Worldwide there are 3 million sudden cardiac deaths per year due to acute myocardial infarction1. World Health Organization has declared cardiovascular disease as a modern epidemic2. Electrophysiological properties of myocardial membrane are associated with major electrolytes like Serum sodium, potassium and calcium. The sarcolemma having Na-K AT Pase pump exports Na from the cell out and imports K inside the cell against their concentration gradient. Thus intracellular K is relatively high and Na is low and extracellular Na is high and K is low. There are 4 phases of action potential dependant on sodium, potassium and calcium. After an episode of acute myocardial infarction serum electrolyte imbalances are common3,4.
MATERIAL AND METHODS Study design: It is a prospective clinical study carried out on cases and controls between 35-70yrs. Study site: the study was carried out at medicine intensive care unit of Dr. Shankarrao chavan Govt. Medical college and Hospital, Nanded. Study population: This study was carried out on 90 patients out of which 45 were cases of MI and 45 were taken as healthy controls with the following criteria: Inclusion Criteria
Exclusion Criteria
Statistical Analysis: For the statistical analysis SPSS package was used in the study. All values were expressed as mean ± SD. For all analysis 'p' value < 0.05 was defined as significant.
RESULTS In our study population, 67% (n=60) were male and 33% (n=30) were female. Out of these 22% (n=20) patients died during first seven days. Amongst the patients died 13% (n=12) were male while 9% (n=8) were female.
Table 1: Showing comparison of serum electrolytes between cases and controls
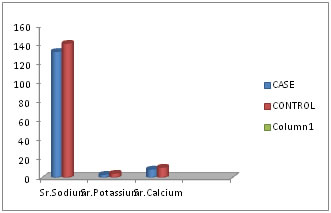
Figure 1: Graphical presentation of serum electrolyte level between case group and control group
DISCUSSION Electrolyte imbalances are fairly common in the acute MI patients. When measured on admission, the sodium, potassium and calcium levels were found to be significantly reduced in our study as compared to non-infarct controls. Mean sodium level of the patients survived was 141.37±5.38 and in patients who died was 132.75±14.19. So, it was found that mortality was higher in patients with hyponatremia. Flear et al showed 45% of infarcted patients had hyponatremia and were associated with increased mortality12. Hypokalaemia was found to be associated with increased risk of ventricular tachycardia in our study and in studies by Dyckner et al and Erik et al13,14. There is a five-fold increase in incidence of ventricular fibrillation in patients with low potassium15. Calcium ions play a vital role in excitation-contraction of the cardiac muscle fibres16.Furthermore hypocalcaemia impairs myocardial contractility and there are several reports of congestive heart failure caused by severe hypocalcaemia17 and cardiomyopathy in long-standing hypocalcaemia18.
CONCLUSION Electrolyte imbalance was maximally seen in Calcium. Hypocalcaemia was present in around half of total cases. Hypokalaemia was present in large number of patients with acute myocardial infarction, mostly due to catecholamines response in such patients. It has been associated with increased mortality in MI patients. From this study we conclude that there was increased mortality in patients with hyponatremia, but p value was non significant.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.