 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 1 - January 2018
Study of uric acid levels among patients with myocardial infarction (MI) attending a teaching hospital
Vasundhara Devi Dundi1, Nagababu Pyadala2,3*, Rathnagiri Polavarapu4
1Associate Professor, 2Assistant Professor, Department of Biochemistry, MNR Medical College and Hospital, Sangareddy, Telangana State, INDIA. 3Research Associate, Department of Clinical Research Laboratory, Genomix Molecular Diagnostics Pvt. Ltd, Kukatpally, Hyderabad, INDIA.. 4President and CEO, Genomix CARL Pvt. Ltd, Pulivendula, Andhra Pradesh, INDIA. Email: nagababu00799@gmail.com
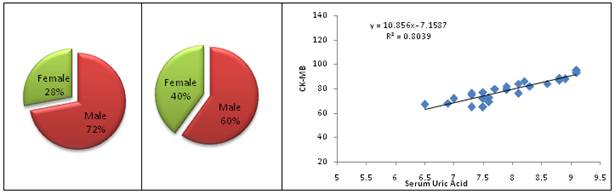
Abstract Aim: The present study aimed to assess the correlation of serum uric acid levels with CK-MB in patients with MI attending a teaching hospital. Methods: A total of 50 study subjects with MI were selected for this study and divided into controls (25 subjects) and cases (25 patients) from the medicine ward of MNR Medical College and hospital, during the period from May 2017 to September 2017. Results: Uric acid levels were compared between the controls and cases. Highly statistical significance observed in the levels of serum uric acid (p<0.0001). Meanwhile, the correlation was done between serum uric acid and CK-MB levels among cases (y = 10.856x - 7.1587, R² = 0.8039) Conclusion: The present study identified that the patients are at high risk with MI those who have the high serum uric acid levels. Serum uric acid had a significant statistical correlation with CK-MB levels in patients with myocardial infarction. The above results of our study showed that hyperuricemia associated with myocardial infarction by promoting vascular dysfunction and coronary thrombosis. Key Words: uric acid levels, myocardial infarction.
INTRODUCTION Globally, Cardio Vascular Diseases (CVD) became one of the leading cause of death. Among CVD, Myocardial Infarction (MI) is the most important form of CVD and continues to be the leading cause of death in the developed and developing countries like India. At present, worldwide 17 million deaths occurred due to the result of CVD. Among total CVDs Coronary Heart Disease (CHD) is an important component and it accounts 25-30% of the death in most developed and developing the country1,2,3,4. Uric acid is a metabolite of purine and functions as an antioxidant. According to Sokhanavar S et al., (5) there is a relation between MI and hyperuricemia. hyperurecemia defined as increased serum uric acid levels more than 7mg/dL and 6mg/dL in women. The uric acid used as a biomarker for inflammation. Recently researchers identified uric acid as a biomarker as an independent risk factor for CHD6,7,8,9,10. Uric acid levels in serum will reflect the xanthine oxidase activity. High levels of uric acid can predict the significant mortality in patients with MI because of Ischemia where the ATP levels are decreased and changed into hypoxanthine a then to uric acid by xanthine oxidase11. Hyperuricemia due to impaired xanthine oxidase activity known to associated with harmful effects on oxidative metabolism, endothelial dysfunction, platelet adhesiveness and aggregation. There are some studies which reported the development of MI in association with hyperuricemia12,13. The present study aimed to assess the correlation of serum uric acid levels with CK-MB in patients with MI attending a teaching hospital.
METHODS AND MATERIALS The present study was carried out at MNR Medical college and hospital situated in Sangareddy, Telangana state. A total of 50 study subjects with MI were selected for this study and divided into controls (25 subjects) and cases (25 patients) from the medicine ward of MNR Medical college and hospital, during the period from May 2017 to September 2017. This study approved by institutional ethical committee and investigations were carried out in the biochemistry laboratory, MNR Medical college and hospital situated in Sangareddy, Telangana state. Inclusion Criteria: Patients who were admitted to medical ward as MI by ECG changes reflecting non-ST elevation MI or ST-elevation MI or, clinical history with increased CK-MB levels included in this study as cases. Exclusion Criteria: The previous history of MI, diabetes mellitus, Hypertension, chronic kidney disease, primary lipidemia, gout and patients under medication like salicylates, ethambutol, Diuretics, Pyrazinamide excluded from this study. Sample collection: Under aseptic conditions, 3ml of venous blood collected into a plain vacutainer after confirming as MI with above inclusion criteria. Whole blood was allowed to clot and then centrifuged for serum separation. Then serum was used to estimation CK-MB and Serum Uric Acid. Statistical Analysis: Data analyzed by statistical tests using SPSS package version number 16. Pearson’s Correlation Coefficient was used to study the relationship between CK-MB and serum uric acid among cases and controls. Data expressed regarding mean ± SD. Unpaired’-test was used to study the changes in the serum uric acid. P-Value < 0.0001 was taken as highly significant. RESULTS In the present study, total 50 subjects divided into two groups, 25 controls and 25 cases with the age range of 35 – 70 years as shown in the table 1 and figure 1and2. Out of 25 controls, 10 were females and 15 males, and in 25 cases, 07 were females and 18 men as shown in the [Table 2 and Figure 3 and figure 4].
Table 1: Age distribution of controls and cases
Figure 1: Age distribution of Cases
Figure 2: Age distribution of Controls
Table 2: Gender wise distribution of study population (n=50)
Figure 3 Figure 4 Figure 5 Legend Figure 3: Gender wise distribution of cases; Figure 4: Gender wise distribution of Controls; Figure 5: Correlation between Serum Uric Acid and CK-MB levels in Cases Table 3: Comparison of Serum Uric acid levels among Cases and Controls
DISCUSSION In the present study, uric acid levels were compared between the controls and cases as shown in table 3. Highly statistical significance observed in the levels of serum uric acid (p<0.0001) (table 3). Meanwhile, the correlation was done between serum uric acid and CK-MB levels among cases as shown in figure 5. Similar studies reported by Nadkar et al.,200813, Sokhanvar S et al.,200714 Jacobs D et al., 197215. According to the studies reported there is a significant increase in the serum uric acid levels in patients with MI and stated that uric acid is a good predictor of mortality in those patients. The activity of xanthine oxidase reflected by serum uric acid levels which contribute the dysfunction of endothelial. High levels of uric acid will stimulate the p38MAP kinase and the nuclear transcription factor AP-1 and NF-Kb, which initiates the synthesis of chemoattractive protein one from monocytes. These chemoattractive proteins are important in causing tissue injury and vascular dysfunction16. Simultaneously platelet aggregation increased along with high uric acid levels and led to the formation of uric acid crystals. Due to the significant deposition of uric acid crystals in the arterial wall would be the reason for the damage of arteries, initiating coronary thrombosis17. So the present study concluded that hyperurecemia is one of the main cause for plaque rupture and responsible for MI.
CONCLUSION The present study identified that the patients are at high risk with MI those who have the high serum uric acid levels. Serum uric acid had a significant statistical correlation with CK-MB levels in patients with myocardial infarction. The above results of our study showed that hyperuricemia associated with myocardial infarction by promoting vascular dysfunction and coronary thrombosis.
REFERENCE
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.