 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 10 Issue 2 - May 2019
Dahire P L1, Ankushe R T2*, Bagade V G3
1Assistant Professor, 2Professor and Head, 3PG Student, Department of Community Medicine, SRTR Government Medical College, Ambajogai, Maharashtra, INDIA. Email: rajtulank@yahoo.com
Abstract Background: Health is pivotal for the growth, development, and productivity of a society and is vital for a happy and healthy life. It has been stated that No Health without mental health. Depression is a disorder of major public health importance, in terms of its prevalence, suffering, dysfunction, morbidity and economic burden. It has been estimated that the burden of depression will increase to 5.75% of total burden of disease and it would be second cause of disability adjusted life years (DALYS) second only to ischasemic heart disease. Objectives: To assess the prevalence of depression in a rural population of productive age group using Patient Health Questionnaire-12(PHQ-12) and to study various risk factors associated with depression. Methods: A community based cross sectional study was planned in field practice area of community medicine department S R T R Government Medical College, Ambajogai, Maharashtra. Systematic random sampling technique was used and a total 216 individuals between 20 to 60 years of age group were interviewed using a pretested structured Patient Health Questionnaire-12 after obtaining informed written consent. Results: Prevalence of depression was 36.57% in study subjects (52.43%Women and 26.86% men).Mild depression was present in 30.09% of study population followed by moderate depression (6.48%) Factors like Female gender, nuclear family, unmarried and others (which includes widowed, divorced, separated), lower socioeconomic status, those having associated co morbid conditions were found to be independent predictors of depression. Conclusion: Depression was found to be more prevalent in females than males in a rural population of productive age group. Depression, more specifically mild depression is a significant problem in rural population which needs to be addressed for effective implementation of mental health promotion. Key Word: Depression, Patient Health Questionnaire-12 (PHQ-12).
INTRODUCTION Health is pivotal for the growth, development, and productivity of a society and is vital for a happy and healthy life. The definition of Health as per the World Health Organization includes physical, social, spiritual and mental health, and not merely an absence of disease or infirmity.1 It has been stated that No Health without mental health.2 This underlines the fact that mental health is an integral and essential component of health. Depression is a common mental disorder, characterized by persistent sadness and a loss of interest in activities that you normally enjoy, accompanied by an inability to carry out daily activities, for at least two weeks.3 Depression is a disorder of major public health importance, in terms of its prevalence, suffering, dysfunction, morbidity and economic burden. It has been estimated that the burden of depression will increase to 5.75% of the total burden of disease and it would be second cause of disability-adjusted life years(DALYs) second only to Ischaemic heart disease.4 Depression was found to be the most common disability in a study conducted by the World Health Organization in fourteen primary care settings worldwide.5Depression is estimated to affect 340 million people globally.6The prevalence of the psychiatric disorder is reported to differ between countries and within countries across various ethnicities.7 In 2013, India accounted for 15% of global DALYs attributable to mental, neurological and substance use disorder(31 million DALYs) with depression accounting for 37% (11.5 million DALYs).8 As per National Mental health Survey 2015-16, the lifetime prevalence of depression in India was 5.25% among individuals aged 18+ years. WHO has declared World Health Day theme for the year 2017 as ‘Depression - Let’s talk’. In India, very few community-based studies have been conducted on depression in rural population of productive age group. With reference to above background, this study was conducted to provide data on the prevalence of depression in a rural population of productive age group using the Patient Health Questionnaire(PHQ-12)and study its associated risk factors. MATERIALS AND METHODS A Community based cross-sectional study was carried out in rural field practice area of Swami Ramanand Teerth Rural Government Medical College, Ambajogai, Maharashtra. Duration of study was3 months from 1st November 2017 to 31st January 2018. Inclusion criteria
Exclusion criteria
Sample size: The Sample size was calculated by using formula , where n= Minimum sample size required for the study, z =1.96, d- absolute precision (d =0.05), p- prevalence, q=1-p and by taking 15% prevalence of depression.9 Calculated sample size was 196. Considering 10% non-response rate, the corrected sample size was 216. Sampling Technique: A total of 216 individuals were selected from our field practice area (sampling frame of 2185 individuals) by using systematic random sampling method and sampling interval of 10. 1st individual is selected from 1st 10 individuals of sampling frame by lottery method and then subsequent individuals were selected at interval of 10 till to get the required sample size of 216. The purpose of the study was explained to participants and written informed consent was taken from them in the local language. Data regarding socio-demographic factors such as age, sex, religion, education, marital status, type of family, occupation, socioeconomic status, and morbid condition etc; was collected using pre-designed and pre-tested proforma. A Tool used for assessment of depression: Depression was assessed by using Patient Health Questionnaire(PHQ-12) whose reliability and validity as a screening tool was tested in Indians.10Patient Health Questionnaire-12 consists of 12 questions with a maximum score of 12. Each question has yes or no responses with 1 score for each yes response. Those who scored 4 or more were considered as having depression. Ethical clearance was obtained from the Institutional ethics committee of our college. Statistical Analysis: Data was compiled and analyzed using Microsoft Excel, Epi Info version-6 software and SPSS-21. Frequency distributions were calculated for almost all independent variables. Odds ratio and its 95% confidence intervals were calculated. Chi-square test was used to determine statistical significance between Depression and independent variables and p< 0.05 was considered to be as statistically significant. Those study participants who found moderate to severe depression were referred to college hospital for psychiatric evaluation and management.
RESULTS TABLE 1: Distribution of study participants according to Socio-demographic characteristics
# Modified BG Prasad Classification * Others includes widow/widower/separated/divorced. Table no 1 showed sociodemographic characteristics of study participants. Out of 216 study participants enrolled in the study, there were 134 males (62.03%) and 82 females (37.96%). The mean age of the study population was 36.6(+11.o1) years. Majority of the study population were Hindu (67.59%), working (93.5%), literate (86.1%), married(80.1%), living in a joint type of family(77.8%) and belonged to upper socioeconomic class(58.4%) as per modified B. G Prasad classification. Table 2: Distribution of Study population on basis of PHQ-12 Score(N=216)
Table 2 shows the distribution of study population as per PHQ-12 SCORE. Out of 216 study respondents interviewed, 79 were having depression as per PHQ12 Score (36 male and 43 female). 30.09%of study population were having mild depression and 06.48% population having moderate depression. No study respondent showed severe depression.
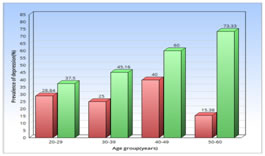
Figure 1: Age-wise and Gender wise distribution of depression in a rural population Above bar diagram showed that the prevalence of depression among female was increased with increase in age but no such trend was observed in the male. Table 3: Risk factors for depression (N=216)
*p value significant Table 3 shows that the females were more likely to suffer from depression as compared to male (p=0.000). The study subjects living in a nuclear type of family were 2.56 times more likely to suffer from depression as compared to those living in a joint type of family(p=0.004). The other variables that had a significant association with prevalence of depression were the lower socioeconomic class (middle class and below), illiterates, those living alone without a spouse i.e., unmarried, widowed, divorced, and presence of other co-morbid conditions. There was no significant association between age (p=0.249), religion (p=0.895), and occupation (p=0.944) and the prevalence of depression.
Table4: Multivariate analysis of the association of risk factors with depression
*p value significant Table 4 shows the result of multiple logistic regression analysis. Multiple logistic regression analysis revealed that in our study population, Female gender, nuclear family, unmarried and others (which includes widowed, divorced, separated), lower socioeconomic status, those having associated co morbid conditions were found to be independent predictors of depression. Age, religion, education status, occupational status was not found to have a significant effect on the prevalence of depression. DISCUSSION As per PHQ-12 SCORE of 4 or more, the prevalence of depression in a rural population of productive age group was found to be 36.57%. The similar result was revealed by study conducted in a rural area of Ahmednagar district, Maharashtra.11 Table 5: Different studies on depression
Table 5 shows different studies on depression from various regions The much lower result was revealed in studies conducted by Sengupta et al (8.9%), Prachet et al (29.36%), Rajkumar et al (12.7%), Taqui et al (19.5%).12-14,18Compared to the present study, the result of other studies was much higher.15-17 Baseline characteristics of the study population, the different tool used for assessment of depression and different sample size might be contributed to this wide variation in the prevalence of depression. Female gender, nuclear family, low socioeconomic status, Illiterate, those living alone without spouse (unmarried/widow/separated/divorced) are associated with depression. Similar findings were observed by Sengupta et al and Kamble et al.11-12 On multiple logistic regression analysis, the present study revealed that Female gender, nuclear family, those living alone without spouse, low socio economic status, associated comorbid conditions were strong predictor of depression where as Sengupta et al observed only female gender and nuclear family as predictor of depression.12 The present study revealed that co morbid condition is associated with depression. A similar finding was seen in Pracheth et al.13 There was no significant association between depression and Gender, co morbid conditions in Goyal et al .17
CONCLUSION The prevalence of depression in a rural population of productive age group was 36.57%. We found that socioeconomic factors and morbid conditions were major risk factors for depression. Depression, more specifically mild depressionis a significant problem in rural population which needs to be addressed for effective implementation of mental health promotion. Such kind of study helps to persuade family physician regarding the importance of early detection and treatment of depression. Early detection is probably the first step in the pathway to manage depression and this need to happen in variety of settings like homes, workplaces, educational institutions, health care and community settings through informed and trained persons.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.