 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 11 Issue 3 - January 2019
Assessment of compliance to anti-rabies vaccination of post exposure prophylaxis among animal bite cases reporting to dedicated anti rabies clinic of a tertiary care hospital, Hassan, Karnataka
G Praveen1, K J Subhashini2*, Siddharam S Metri3, M Sundar4
1Associate Professor, 2Postgraduate, 3Assistant Professor, Professor and HOD, Department of Community Medicine, Hassan institute of Medical Sciences, Karnataka, INDIA. Email: dr.subhashini215@gmail.com
Abstract Background: Rabies, a neglected tropical disease which is 100% fatal yet preventable by proper and adequate Post-Exposure Prophylaxis (PEP) which includes wound wash, full course of anti-rabies vaccination (ARV) and wound infiltration of rabies immunoglobulin in all category III bites. It is essential for the bite victims to complete the full course of vaccination as recommended to prevent rabies. Objectives: To determine the patient’s compliance for intradermal ARV and the constraints for non-compliance among animal bite cases reporting to dedicated Anti-rabies clinic (ARC) of a tertiary care hospital, Hassan, Karnataka. Methods: A Longitudinal study was conducted from October 2017 to August 2018. All the animal bite victims fulfilling the inclusion and exclusion criteria reporting to Anti-Rabies Clinic (ARC) were followed-up to know the compliance for complete course of ARV using Updated Thai Red Cross Regimen. Reasons for non-compliance were asked to the animal bite victims who discontinued vaccination against recommendation through telephonic communication on the 30th day of their schedule. Descriptive statistics employed. Results: All the animal bite victims of category II and III who reported to ARC were given the 1st dose of ARV. The compliance rate for 2nd dose was 94.1% and decreased subsequently for 3rd (87.5%) and 4th dose (50.3%). The reasons for non-compliance were found as transportation problems, loss of wages, non-availability of rabies biologicals in Peripheral centres, negligence and forgotten dates. Conclusion: This study emphasis the need for motivating the animal bite victims in completing the full course of vaccination and constraints for non-compliance need to be addressed by the policy makers. WHO recommended shorter duration vaccination schedule could be implemented to reduce non-compliance among the animal bite victims. Key Words: Compliance, Constraints, Post-exposure Prophylaxis, Zoonoses.
INTRODUCTION Animal bites cause a big burden in terms of morbidity and mortality globally. As per the World Health Organization (WHO), the dog bites are the cause for tens of millions of injuries annually, followed by snake bites, cat bites and monkey bites.1 According to WHO-APCRI National Multi-centric Rabies Survey, there are an estimated 17.4 million animal bite cases annually in India.2 These animal bites could be caused by rabid animals that results in the highly fatal disease, Rabies.3 Every 2 seconds, a person is bitten and every 30 minutes, someone dies from rabies.4 Rabies is the 10th biggest cause of death due to infectious diseases globally. Every year about 59,000 die of rabies, of which 20,000 are from India alone which constitutes one-third of rabies deaths.5,6 Though rabies being a 100% fatal disease, it is also 100% preventable.7 by following proper and adequate Post Exposure Prophylaxis (PEP). PEP is considered of monumental importance in prevention of rabies.8 PEP consists of thorough wound washing with soap and water, Anti-rabies vaccination (ARV) and timely administration of Rabies immunoglobulin (RIG) for category III bites.9 In India, Updated Thai Red Cross regimen of Intradermal vaccination (2-2-2-0-2) is adopted.10 Timely and complete PEP for these animal bite victims is necessary to prevent rabies. Therefore, the attending anti-rabies clinic (ARC) physician must provide appropriate PEP and it is also essential for the bite victims to complete the full course of vaccination as recommended.11 However, the importance of completion of the schedule is often ill-conceived and neglected probably because rabies not being included in the list of notifiable diseases.8,12 And many a times people do not take the complete course of vaccination and some of the noted reasons for non-compliance like loss of wages, forgotten dates, cost incurred and distance from the hospital that prevents patients from taking all doses of ARV.12 In order to prevent rabies deaths, the Global Alliance for Rabies Control (GARC) have put forward the global strategic plan “Zero by 2030” to reduce the human deaths from rabies to zero by the year 2030 13. India is also trying to take steps in achieving this goal of zero-rabies mission through National Rabies Control Programme under the Ministry of Health and Family welfare.14 The District Health and family welfare, Hassan, Karnataka is trying to implement the Rabies control programme in Hassan district. Hence understanding the compliance to the PEP and the constraints for non-compliance helps the Programme officers in effective implementation of the programme in the district.
OBJECTIVES To determine the patient’s compliance for intradermal Anti - Rabies Vaccination and to describe the constraints for non-compliance among animal bite victims reporting to dedicated Anti-rabies clinic of a tertiary care hospital, Hassan, Karnataka.
MATERIALS AND METHODS The Dedicated Anti-Rabies Clinic (ARC) was started under the Department of Community Medicine, Government Medical College, Hassan on October 12th, 2017. Management of animal bites except snake bites are exclusively provided in dedicated Anti-Rabies Clinic. Anti- Rabies Vaccination (ARV) and rabies immunoglobulin (RIG) for prevention of rabies are being provided completely free of cost to all victims irrespective of their socio-economic status. On an average, 15-20 animal bite cases are being reported daily for treatment. Postgraduates and interns are posted to Anti-Rabies clinic on a regular basis. The cases are educated by the treating physician routinely on the importance of completing the full course of ARV to prevent rabies as it is 100% fatal yet preventable. IEC materials are displayed in the ARC and cases are educated with those materials by the treating physician. A Longitudinal study was conducted from October 12th, 2017 to August 31st, 2018 including all the animal bite cases reporting to Anti-Rabies Clinic. Patients visited the dedicated ARC of the District hospital not only from the Hassan taluk but also from all the other seven taluks of Hassan for treatment of animal bites because of the non-availability of rabies biologicals in their area. Hence, all the patients who attended the dedicated ARC were included in the study and were followed up for the completion of the course. Inclusion criteria: All the animal bite victims irrespective of age and animal bite victims with mobile phones or landline phones for communication were included in the study. Exclusion criteria: Rat bite, Rabbit bite, Rodent bite, snake bite and human bite cases; cases who came for pre-exposure prophylaxis and re-exposure prophylaxis; those who were critically injured and not able to respond.
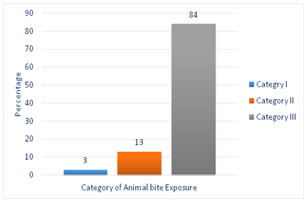
METHODOLOGY Ethical clearance was obtained from Institutional Ethical Committee. Informed verbal consent was sought from the study participants and assent from those below 18 years of age. The animal bite victims fulfilling the inclusion and exclusion criteria who attended the anti-rabies clinic during the study period were found to be 3500. They were interviewed by using a semi-structured, pre-designed and pre-tested, closed ended proforma that included data regarding socio-demographic profile and compliance to PEP was noted through interview. The patients’/ relatives’/guardians’ phone number was also recorded for all patients who attended the Anti-Rabies Clinic. The patients were categorized according to WHO Categorization of contact with suspected animal bites into Category I, II, III. All animal bite victims belonging to category II and III who require PEP were given ARV and all category III victims were provided rabies immunoglobulin. They were followed-up till their last dose to know the compliance for complete course of ARV using Updated Thai Red Cross Regimen (2-2-2-0-2) i.e., 0.1 ml × 2 sites intradermally on days 0, 3, 7, and 28.15 The animal bite victims who discontinued the vaccination at any point during the recommended course were considered as noncompliant bite victims and those who discontinued vaccination after 3 doses, where the animal remains healthy and alive for a least 10 days after the exposure were considered as compliant bite victims. Reasons for non-compliance were asked to the patients through telephonic communication on the 30th day of their schedule. Individual responses were collected from the cases as narrated and later they were categorized into various reasons of non-compliance for the purpose of analysis. Patients who do not respond through telephones even after 3 times of calling them were considered as non-responders. Statistical Analysis: Data entered in Microsoft Excel 2016 and analyzed using SPSS version 20. Descriptive statistics was employed for data analysis and depicted as proportions and percentages. Chi Square test for trends was employed to find any significant differences in association over time between ordinal independent categorical variables and binomial dependent variable. Results depicted as tables and graphs. OBSERVATION AND RESULTS All the animal bite victims irrespective of age who attended the anti-rabies clinic during the study period were found to be 3500. Rat bite, Rabbit bite, Rodent bite, snake bite and human bite cases were excluded as they do not require ARV or RIG. Those patients belonging to Category II and III who received ARV were followed up to know the compliance. In this study, 47.3% of the animal bite victims belonged to the age group of 20- 50 years. The proportion of animal bite cases less than 19 years old were 30.4%. Majority of the animal bite victims were males (66.2%) and females constituted 33.8%. Majority belonged to the rural population (77.0%). Most of them (62.3%) belonged to Lower socio-economic status followed by Middle (35.6%) and Upper (2.1%) classes classified according to Modified B.G Prasad classification 2018 [16]. Graph 1: Distribution of study subjects based on categorization of animal bite (n=3500)
Graph 1 shows the distribution of animal bite victims categorized according to WHO classification of animal bite exposures. 105 (3.0%) belonged to category I, 455 (13.0%) belonged to Category II and 2940 (84.0%) belonged to Category III. In this study, only 33.0% of the animal bite victims have taken all the 4 doses of ARV, 54.4% have taken three doses whereas 5.9% of the subjects have taken only one dose of ARV.
Table 1: Compliance to intradermal Anti-Rabies Vaccination of Post-Exposure Prophylaxis
Figures in the parenthesis indicate percentage (%); *Chi square for trends: p = <0.001.
Table 2: Reasons for non-compliance to complete course of Anti-Rabies Vaccination
Figures in the parentheses indicate percentages (%)
All the patients of category II and III (n=3395) were given the first dose of ARV (Day 0). They were followed up throughout the entire course of the schedule to know the compliance to Anti-Rabies Vaccination. Majority (94.1%) of the animal bite victims reported for the second dose and 87.5% of the subjects reported for taking the third dose. But only 33% of the bite victims reported for taking the last dose of ARV. The compliance to anti-rabies vaccination declined significantly with each subsequent dose. (Chi square for trends: p<0.001). (Table 1) The patients who reported for third dose of ARV were enquired about the status of the animal if it remained healthy/ alive and advised to observe the animal for 3 more days. 740 of those 2969 patients (Day 3) reported healthy status of the animal and animal was available for observation. Hence they were advised to omit the fourth dose. And the remaining 2229 patients were expected to take 4th dose of ARV and out of them 1121 had taken the dose. Hence the compliance rate for 4th dose was 50.3% (95% CI 48.2 – 52.4%) In our study, only 1121(33%) out of 3395 patients had taken all the four doses of ARV. The remaining 2274 (77%) who were non-compliant were communicated through telephone to know the reasons for not reporting to the dedicated Anti- Rabies clinic on the scheduled dates for ARV. As advised by the treating doctor, 740 patients discontinued the 4th dose as animal was available for observation and was healthy. Hence these 740 patients were considered compliant. The patients who completed their schedule in private clinics were 57 and hence not considered non-compliant. The patients who could not be contacted even after 3 times of telephonic communication were 296 and hence they were considered non-responders. Hence remaining 1181 patients were asked for constraints for non-compliance. Table 2 summarizes the constraints reported by the patients for non-compliance.
DISCUSSION Rabies is a 100% preventable disease. Nearly 80% of human rabies deaths in India had occurred because the animal bite victims had not received proper and adequate Post Exposure Prophylaxis. Therefore, in India which is endemic for rabies, every animal bite should be treated as a rabid animal bite and appropriate post-exposure prophylaxis should be strictly followed.15 In this study, majority of the animal bite victims belonged to the age group of 20- 50 years followed by those less than 19 years. Majority of the animal bite victims were males and most of them were from lower socio-economic status. Majority of the animal bites belonged to category III. This is similar to other studies done across the country by Sreenivas NS et al.7 in Bangalore, Shankaraiah RH et al.11 in Bangalore, Ravish HS et al.15 in Bangalore, Anandaraj R et al.16 in Davangere, Gudegowda KS et al. 17 in Bangalore, and Domple VK et al.18 in Maharashtra. Increased prevalence of animal bites among males and poor population may be probably because of extensive outdoor activities when compared with their counterparts. In our study, majority belonged to the rural population in contrary to the studies done by Sreenivas NS et al.7, Shankaraiah RH et al.11, Ravish HS et al. 15, Gudegowda KS et al.17 but all these studies were conducted in an urban background but the WHO’s latest technical report series quotes that increased occurrence of animal bite cases are found in rural areas.6 In this study, 33% of the animal bite victims had taken all the four doses of ARV. But an additional 740 animal bite victims had been advised to discontinue the schedule after third dose as the biting animal was healthy and available for observation. Hence the compliance to full course of ARV increases to 54.8%. Similarly, previous studies conducted by Mahendra BJ et al.19 and Vinay et al.20 showed a compliance rate of 38.5% and 35% respectively which is relatively less compared to the present study and also the studies done by Manna N et al.7, Shankaraiah RH et al.11, Bariya BR et al.21 and Satapathy DM et al.22 showed a compliance rate of 70.5%, 77%, 70% and 65% respectively which shows increased compliance to ARV schedule. In our study, the compliance to 2nd dose was 94.1%, to 3rd dose was 87.5% and to the last dose was 50.3% considering that 740 patients who have been advised to discontinue the 4th dose. This wider discrepancy between the 3rd and the 4th dose may be attributed because of the comparatively longer interval (21 days) between the third and the fourth dose. In a study done by Shankaraiah RH et al.11 in Bangalore the compliance to 1st, 2nd, 3rd and 4th dose was found to be 100%, 91.9%, 88.1% and 77%. Another study by Gudegowda KS et al.17 shows the compliance to be 89.2%, 72.1%, 65.1% and 61.5%. Other study by Malkar et al.23 showed as 100%, 82.9%, 70.1% and 46.2%. These studies also show as the dose increases, the number of patients reporting for ARV decreases. Our study shows a greater difference in compliance between 3rd and 4th dose rather than between first and second; second and third doses. This focuses on the need for validated shorter duration ARV schedules for better compliance among animal bite victims. WHO technical report series on Rabies, 2018 has suggested alternative one week, two sites, intradermal PEP regimen (2-2-2-0-0) on day 0, day 3 and day 7 instead of 2-2-2-0-2 on days 0,3,7 and 28. This suggestion have been made after assessing for immunogenicity, clinical outcome, feasibility and cost-effectiveness of the intradermal anti-rabies vaccines.6 The reasons for non-compliance reported by non-compliant animal bite victims were transportation problem, loss of wages, non-availability of rabies vaccines and other biologicals the nearby Primary Health Centres, unawareness regarding the importance of taking the full dose of ARV, dates have been forgotten, completing the ARV schedule in nearby private clinics who were affordable and interference with school/work timings. Similarly, studies by Shankaraiah RH et al.11, Gudegowda KS et al.17, Mahendra BJ et al.19 and Bariya BR et al.21 also highlights some of these issues. The rabies vaccines and immunoglobulins are not routinely available in the peripheral health care units because of the limited availability and supply of PEP. Stock-outs are frequent, due to either low budg et al location for rabies biologicals at central level, ineffective use of PEP at treatment centres and/or lack of accurate vaccine forecasting6 As most of our animal bite victims belonged to rural population in our study, it highlights the importance of adequate and regular supply of rabies biologicals in PHCs/CHCs. That will also address the other issues said by the non-complaints like transportation problem to district hospital and loss of wages.
CONCLUSION This study highlights that the compliance to 2nd dose was 94.1% and decreased subsequently for 3rd dose (87.5%) and 4th dose (50.3%). This highlights the importance of having authenticated shorter duration ARV schedules for better compliance towards vaccination. The reasons for non-compliance were found as lack of awareness, loss of wages, transportation problems, non-availability of rabies biologicals in PHC and forgotten dates. The programme officers and other health care personnel have to understand the constraints for non-compliance and address those issues for effective prevention of rabies.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.