 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 - April 2019
Study on aerobic bacteriology in chronic suppurative otitis media: A hospital based prospective study
Chethan Kumar G1, Kiren T2*, Gopakumar3, Adhavan E4, Kingsly S5
1Associate Professor, 2Assistant Professor, 3Professor and HOD, 4,5Junior Resident, Department of ENT, Sree Mookambika Institute of Medical Sciences, Kulasekharam, Kanyakumari (Dist), Tamil Nadu, INDIA. Email: kiren21t@gmail.com
Abstract Background: Chronic Suppurative Otitis Media (CSOM) is a disease of multiple etiology posing a major health problem in developing countries causing serious local damage and threatening complications. Early treatment is based on the type of microorganism infection. This study was aimed to study the aerobic bacteriology in CSOM. Materials and Methods: This study was conducted in the Department of ENT, Sree Mookambika Medical College, Kulasekharam, Tamil Nadu. 100 patients with CSOM were included in the study. The patients had chronic ear discharge and had not received antibiotics for the last seven days. Swabs were taken and cultured for microbial flora. Drug susceptibility testing for aerobic isolates was conducted by Kirby-Bauer’s disc diffusion method. Results: Out of 100 patients, 88 were diagnosed with mucosal disease and 12 squamosal disease. Analysis of this study showed predominance of Gram negative organisms (60%). The highest incidence was that of Pseudomonas aeruginosa (42%), followed by Staphylococcus aureus (21%). Conclusion: Knowing the aetiological agents of COM and their antibiotic susceptibility is important in effective treatment and prevention of both complications and development of antibiotic resistance and finally cost effective management. Key Word: Ear, microorganism, infection, chronic otitis media, gram negative bacteria.
INTRODUCTION The assessment and management of chronic suppurative otitis media (COM) presents many challenging and fascinating problems. The state of individual ear involved in chronic disease represents the balance established at a particular time between the progression of the disease process and the healing response within the middle ear cleft. Accordingly the manifestations of chronic suppurative otitis media are extremely variable and there may be any lesion from a small healed deformity of the tympanic membrane, to a cholesteatoma infiltrating widely throughout the temporal bone1. Chronic suppurative otitis media is a disease of multiple etiological factors and is well known for its persistence and recurrence in spite of treatment. Chronic suppurative otitis media may be defined as a long standing inflammatory disease affecting middle ear muco-periosteal lining. It is a persistent disease with irreversible sequelae and can proceed to serious intra and /or extra cranial complications2. Chronic otitis media equates with the classic term chronic ‘suppurative’ otitis media and that is no longer advocated, as COM is not necessarily a result of the gathering of pus. COM is classified into two types, Tubotympanic (TTD) and Atticoantral (AAD). It has been now replaced by new terminology; Mucosal and Squamous types. Bacteriologically and etiologically, both types are different. Mucosal type is usually a result of incompletely treated acute suppurative otitis media or recurrent suppurative otitis media. Important feature of this type of disease is the presence of central perforation; however, in squamous type, perforation is either marginal or attic3. The incidence of chronic otitis media appears to be dependent on racial and socio-economical factors. The basis for the wide spread prevalence of chronic otitis media has been directed towards socio-economic factors such as poor nutrition and hygiene and poor living conditions like overcrowding. The aim of present study is to find the organisms responsible for chronic otitis media by taking the ear swab.
MATERIALS AND METHODS Study settings and Period: This is a prospective cross sectional study conducted in the Department of ENT, Head and Neck Surgery at Sree Mookambika Institute of Medical Sciences, Kulasekharam from April 2015 to September 2016 after ethical committee clearance from the institution. Inclusion criteria
Exclusion criteria
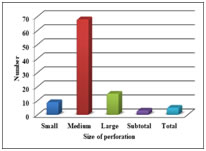
Procedure: A total of 100 patients were included in this study on the basis of inclusion and exclusion criteria. The selected patients demographic data was collected. Ear discharge is collected under aseptic precautions in clinically diagnosed cases of COM. Under microscope, excess discharge is sucked out of the external acoustic canal. Then using a swab that is small and sterile, specimen is collected through the perforation and sent for microbiological analysis. Statistical analysis: The data was expressed in number and percentage. Chi square test applied to find the statistical significant between the groups. p value less than 0.05 considered statically significant at 95 % confidence interval. RESULTS Out of 100 patients analysed, COM was found to be predominant in males (68%) than females (32%). Out of 100 patients, COM was found common among age groups of 6-20 years (62%), which shows predominance of COM in student population. Out of 100 patients in this study, 51% patients presented with complaints of both ear discharge and hearing loss. 33% patients complained of ear discharge only, and 16% had complaints of hearing loss only. Out of the 100 patients in this study, most of the patients had central perforations. Out of 100 patients in this study, most patients had medium sized perforations (68%). Out of the 100 patients, 93% cases showed Rinne’s test negative on the affected ear, 93% Weber’s test lateralized to the affected ear and 81% cases Absolute bone conduction test was normal. In 7% of the patients, tuning fork tests couldn’t be assessed as they were children in lower age group. Absolute bone conduction was found to be reduced in older age group (12%). Out of the 100 patients in this study, 56% of patients showed mild hearing loss (26dB–40dB) in pure tone audiometry, moderate hearing loss (41dB–55dB) in 29% of patients and moderately severe and severe hearing loss in 6% and 2% patients respectively. Pure tone audiometry couldn’t be assessed in 7% of patients as they were children belonging to lower age group due to inconsistent responses. Out of the 100 patients in this study, 88% were diagnosed with Mucosal disease and rest 12% was diagnosed with Squamosal disease. Out of the 100 patients in this study, 60% organisms isolated were Gram negative, Gram positive in 30% and Gram staining was not done in 10% as culture showed commensals or no growth. Out of the 100 patients, most commonest organism was found to be Pseudomonas aeruginosa (42%), followed by Staphylococcus aureus (21%), Klebsiella (9%), Proteus (5%), Coagulase negative staphylococcus aureus (5%), Acinetobacter (4%) and Escherchia coli (4%). There was no growth in 8% of patients and commensal was found in 2%.
Table 1: Demographic data of study population
Table 2: Quadrants of perforation in CSOM
Table 3: Tuning fork test in CSOM
Table 4: Prevalence of microorganisms
DISCUSSION Chronic otitis media (COM) is a chronic infection of the middle ear which can even lead to deafness. Poorly or untreated COM can lead to a number of intra /extra cranial complications. Hence diagnosing the causative organisms is mandatory for proper and successful management of COM. Due to changing pattern of bacteriological profile of otitis media and sensitivity of microorganisms towards antibiotics, it has become very important to find out the organism causing the disease. Hundred patients with chronic otitis media of all age groups of both gender attending the out-patient department and those admitted in ENT ward, who fulfill the criteria of inclusion were selected randomly for the study in the Department of ENT at Sree Mookambika Institute of Medical Sciences. The gender distribution among patients with chronic otitis media in the current study is (68%) males and (32%) females. The male and female ratio is 2:1, suggestive of male preponderance and is comparable with studies done by Vijaya D in 2000 which showed male predominance of 62.77%4. The present study shows that, chronic otitis media is found to be more common among student population (65%) and is comparable with studies done by V K Srivastava et al in 1979 which shows that the common age group in CSOM is 10-14 years [5], J Gulati et al in 1969, stated that common age group is 0-10 years, which shows high incidence in the student population6. The present study showed that chronic otitis media is found common between the age groups of 6-20 years (62%) followed by 21-30 years and is comparable with studies done by J. Gulati et al in 1969, found that the incidence of CSOM is maximum in age group of 0-10 years. Among patients studied, majority presented with ear discharge and loss of hearing (51%) and majority of patients presented with ear discharge of 1- 3 years of duration (45%) and is comparable with previous studies done by J Gulati et al in 1969, which showed that the duration of ear discharge varies from 6 weeks to 10 years. Most patients with COM in the current study showed central perforation and is comparable with the studies done by B M Ahmad et al in 2003, in a retrospective study of patients with CSOM, most common tympanic membrane perforation was of central type which was seen in 60.7% of the patients7. This study showed that majority of patients had moderate size perforation (68%) followed by large size perforation (15%). Major population of patients in the present study had Rinne negative on the affected ear (93%), Weber is lateralized to the affected ear (93%) and Absolute Bone Conduction is normal in (81%). In 7% cases couldn’t access the tuning fork tests as they were children in lower age group. ABC is reduced in older age group (12%). Pure tone audiometry done in the present study showed, 56% of the patients with chronic suppurative otitis media has mild hearing loss (26- 40db) and 29% has moderate hearing loss (41-55db). In 7%, PTA could not be assessed as they were children in the lower age group. Majority of the patients in the present study are with Mucosal (88%) and 12% were with Squamosal type and is comparable with study done by Kabir MS in 2012, in a study pattern of CSOM among 110 patients, 90% patients presented with TTD and 10% patients presented with AAD8. Radiological assessment was done with either X-ray Mastoid or HRCT Temporal bone in only patients with squamosal disease of those who were planned for surgery and out of it 11% showed cholesteatoma cavity with bony erosion and scelorosis of the mastoid. According to the present study, Gram staining of the organism isolated showed Gram negative organisms in majority of the case (60%) and Gram positive organisms in 30%. Pseudomonas aeruginosa is the predominant organism which is comparable with previous studies done by, Poorey V.K. et al in 2002 which suggested that, Pseudomonas is the predominant organism followed by Klebsiella2. Tanmoy Deb et al in 2012, studied the bacteriological profile of CSOM, suggested that commonest bacteria involved is gram negative bacteria especially the pseudomonas9. In the present study, the commonest organism found in the culture is Pseudomonas aeruginosa (42%) followed by Staphylococcus aureus (21%). The next comes Klebsiella (9%), Proteus and CNSA (5%) each and Acinetobacter and E.coli (4%) each. There was no growth in (8%) and (2%) are commensals and is comparable with previous studies done by, Fliss DM et al in 1992, found that Pseudomonas aeruginosa was the most common isolate. In 48 cases (38%) it was the only isolate. Enteric bacilli, Staphylococcus aureus, Streptococcus and Hemophilus influenzae were also found10, Atanu Nandy et al in 1991, came to a conclusion in a bacteriological study CSOM a total of 146 cases of CSOM (CSOM), comprising of 77 males and 69 females in different age groups were studied. Out of the total 192 isolates, Pseudomonas species ranked highest with 43.8% incidence followed by Staphylococcus pyogenes (18.2%), Proteus sp (12%), Klebsiella sp (7.3%) and Diphtheroides (6.7%)11. Erkan M et al in 1994, in a study of Bacteriology of CSOM, Pseudomonas aeruginosa was recovered mainly followed by Staphylococcus aureus and Klebsiella pneumonia12. RS Greval et al in 1996, in a study on Bacteriological patterns of CSOM, in Ludhiana, concluded that series of 300 cases of CSOM encountered in Dayanand Medical College and Hospital, Ludhiana was surveyed for type specificity to determine latest trends of bacterial prevalence in Ludhiana, Punjab, Pseudomonas, Staphylococcus and Proteus head the list13. Gupta V et al in 1998, In a study of 334 adult patients with CSOM, the commonest organisms isolated were P.aeruginosa while S.aureus were found in CSOM with cholesteatoma³. Indudharan R et al in 1999, in his study on Antibiotics in CSOM and bacteriological study, P.aeruginosa was the major isolated organism (27.2%) followed by S.aureus (23.6%) 14. The early diagnosis plays major role in the treatment of CSOM.
CONCLUSION Chronic otitis media is the most common ear disorder. Most common microorganisms are gram negative. Early detection of congestive organism plays important role in the management of diseases. Administration of specific and selective anti-microbial agents is more useful to control the infection.
REFERENCES
|
|
 Graph 1:
Graph 1: 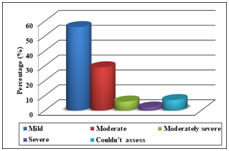 2: Pure tone audiometry in CSOM Graph 3: G
2: Pure tone audiometry in CSOM Graph 3: G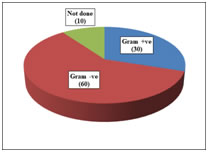 ram staining in CSOM
ram staining in CSOM This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.