 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 - April 2019
P M Hippargekar1, S V Bhise2*, Priyanka V Gurjar3
1Professor and Head, 2Associate professor, 3Junior resident 3, Department of ENT, SRTR GMC Ambajogai, Maharashtra, INDIA. Email: pmhippargekar@yahoo.com bhisesudhir13@gmail.com piagurjar7@gmail.com
Abstract Background: Sinusitis is defined as inflammation of mucosa of paranasal sinuses. According to Bernstien, chronic sinusitis is a residual retention of purulent secretion, within the cavities, with subsequent degenerative, fibrotic and cystic changes. It is invariably associated with nasal polyp and deviated nasal septum. The Task force has Classified rhinosinusitis based upon duration of illness as acute, subacute, recurrent acute and exacerbation of chronic state. Amis and objectives: To study the Correlation of anatomical variations of nasal osteomeatal complex with sinusitis among the patients having nasal septal deviation. Materials and method: In the present study all the symptomatic patients having nasal septal deviation attending the department of ENT during the period of September 2016 to October 2018 were selected for the study. total 100 cases were enrolled in the study with informed consent for participation. Detailed history and clinical examination was done with nasal speculum and nasal endoscope and the grade and type of septal deviation according to Mladina classification was classified and other abnormalities in osteomeatal complex were noted. All the patients underwent radiological investigation which include X-ray PNS and CT PNS. The collected data was recorded in pretested proforma and Statistical analysis was done. of septal deviation with anatomical variation and sinus pathological study was carried out using appropriate statistical tests. Results: The mean age of the study subjects was 30.19±7.94yrs. Majority of the patients were male with male to female ratio of 1.9:1. The most common presenting symptom observed in the present study was nasal obstruction (90%) which was followed by nasal discharge (72%), headache (48%), hyposmia (12%) and nasal bleeding (5%). Severe septal deviation was more frequently associated with sinusitison same side cases (44%). The association of severity sep tal deviation with sinusitison same side was statistically significant. While there was no significant association of septal deviation with sinusitison opposite side was observed. Conchabullosa was observed in 55% cases of which lamellarconcha was seen in 22% case. Bulbous and extensive conchabullosa was seen in18% and15% case seachof these concha associated with sinusitison same side. There was not significant association between the type of conchabullosa and sinusitison same side of disease. There was no significant association between anatomical variation and sinusitison same side and on opposite side also Conclusion: There was a significant association of septal deviation with the sinusitis on same side while there was not significant concha bullosa and its association with sinusitis on same side. The association of other anatomical variation and sinusitis on same side was not significantly associated. Key Word: nasal osteomeatal complex, anatomical variations, sinusitis
INTRODUCTION Sinusitis is defined as inflammation of mucosa of paranasal sinuses. According to Bernstien, chronic sinusitis is a residual retention of purulent secretion, within the cavities, with subsequent degenerative, fibrotic and cystic changes. It is invariably associated with nasal polyp and deviated nasal septum. The Task force has Classified rhinosinusitis based upon duration of illness as acute, subacute, recurrent acute and exacerbation of chronic state.1 The two cardinal factors in the maintenance of normal physiology of the nose and paranasal sinuses are drainage and ventilation. Normal drainage depends on effective mucocilliary clearance; this is dependant, among other things, such as the condition of the sinus ostia, its inflammation and obstructive anatomical variations in nasal cavity. Mucus transport from the sinuses into the nose is greatly enhanced by unimpeded nasal airflow creating negative pressure within the nasal cavity during inspiration.2 Chronic rhino sinusitis (CRS) is the most common disease for which consultation of otorhinolaryngologist is sought. The approach to patients with chronic rhino sinusitis has changed after Messerklinger published the first comprehensive account of technique of nasal endoscopy and its application to the diagnosis and treatment of sinonasal diseases.3 The blockade in osteomeatal complex leads to impaired drainage of maxillary, frontal and anterior ethmoid sinuses that causing sinusitis. The endoscopic surgery aims at removing the obstruction of the main drainage pathway- in the osteomeatal complex-based essentially on the concept that such obstruction perpetuates the sinus disease. The key underlying concept behind minimally invasive functional endoscopic sinus surgery is the osteomeatal complex (OMC) – the small compartment located in the region between the middle turbinate and the lateral nasal wall in the middle meatus. The osteomeatal complex area is encompassed by Ostium of the maxillary sinus, the ostia of the anterior and middle ethmoidal air cells, frontal recess, the ethmoidal infundibulum and middle meatus. And the sphenoethmoidal recess and the superior meatus, these have also been referred as anterior and posterior osteomeatal complex units, respectively.4Stammberger et al5 proposed that stenosis of the osteomeatal complex from either anatomical configuration or hypertrophied mucosa can cause obstruction of secretions that may become infected and perpetuate infection leading to sinusitis/ rhinosinusitis. CT and nasal endoscopy have been used successfully as diagnostic modalities in sinus disease. The purpose of these investigations is to determine the mucosal abnormalities and bony anatomic variations of paranasal sinus and assess the possible pathogenicity of these findings in patients undergoing evaluation for sinusitis. This also prevents occurance of complication in functional endoscopic sinus surgery.6 Thus the present study aims to evaluate the anatomical variation of osteomeatal complex and sinusitis in patient with deviated nasal septum with the help of finding on nasal endoscopy and CT scan. AMIS AND OBJECTIVES To study the Correlation of anatomical variations of nasal osteomeatal complex with sinusitis among the patients having nasal septal deviation.
MATERIALS AND METHOD The present observational study was conducted in the department of ENT of tertiary care institute with the aim to study the Correlation of anatomical variations of nasal osteomeatal complex with sinusitis. Following inclusion and exclusion criteria was used to select the study subjects. Inclusion Criteria:
Exclusion Criteria:
By using the above mentioned inclusion and exclusion criteria total 100 patients suffering from nasal septal deviation were enrolled in the study and informed written consent was obtained. Detailed history was taken and the findings were recorded on a pretested and prestructured proforma. Clinical examination was done with nasal speculum and nasal endoscope and the grade and type of septal deviation according to Mladina classification was classified and other abnormalities in osteomeatal complex were noted. All the patients underwent radiological investigation which include X-ray PNS and CTPNS. In CT scan was performed to determine the mucosal abnormalities and osteomeatal complexvariation of paranasal sinuses, to measure the angle of nasal septal deviation. Presence of anatomical variations pertaining to osteomeatal complex were noted and presence orabsence of sinus pathology was also recorded. The collected data was recorded in pretested proforma. Statistical analysis of septal deviation with anatomical variation and sinus pathological study was carried out using appropriate statistical tests. RESULTS Table 1: Distribution of cases according to age and gender
It was observed that out of 100 cases, majority of the patients were in age group of 21-30 years (55%), followed by 31-40 years (30%).The mean age of the study subjects was 30.19±7.94yrs.It was seen that majority of the patients were male with male to female ratio of 1.9:1. Table 2: Distribution of cases according to presenting symptoms in deviated nasal septum
* Multiple responses were obtained. The most common presenting symptom observed in the present study was nasal obstruction (90%) which was followed by nasal discharge (72%), headache (48%), hyposmia (12%) and nasal bleeding (5%).
Table 3: Distribution of cases according to relation of septal deviation and sinusitis
It was seen that severe septal deviation was more frequently associated with sinusitison same side cases (44%). Among the moderate septal deviation, sinusitison the side of septal deviation was observed in27%cases. The association of severity septal deviation with sinusitison same side was statistically significant. The relation of type of septal deviation and presence of Sinusitis on opposite side was also compared and it was observed that severe septal deviation was associated with sinusitison opposite side in 10% cases. There was not significant association of septal deviation with sinusitison opposite side was observed. Table 4: Distribution o fcases according to types of conchabullosa and its relation withs inusitis
[*CB- conchabullosa, #In cases of bilateral disease each side was assessed for type of conchabullosa and its association withs inusitis] In present study, conchabullosa was observed in 55% cases of which lamellarconcha was seen in 22% case. Bulbous and extensive conchabullosa was seen in 18% and 15% cases each of these concha associated with sinusitison same side. There was not significant association between the type of conchabullosa and sinusitison same side of disease [Chi-square test=3.57, DF=2, pvalue>0.05].
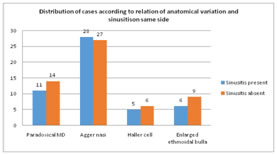
Table 5: Distributionofcasesaccordingtorelationofanatomicalvariationandsinusitis
It was seen that there was no significant association between anatomical variation and sinusitison same side[Chi-square test=0.73,DF=3,P>0.05].
Table 6: Distributionofcasesaccordingtorelationofanatomicalvariationandsinusitis
There was no significant association between anatomical ariation and sinusitison opposite side[Chi- square test=4.77, DF=3, P>0.05].
DISCUSSION The present study was conducted in the department of ENT of tertiary care institute including 100 patients diagnosed as deviated nasal septum between the period of September 2016 to October 2018. Their clinical features, endoscopic and CT scan findings were studied in details as per pre-test proforma. In present study maximum patients with deviated nasal septum (55%) were between age group 21-30 years, followed by 31-40 years 30%.The mean age of the study subjects was 30.19±7.94yrs. Similar findings were, Jane JY et al,7 where mean age of study subjects was 31.5 years, Guyuron B et al,8 observed mean age of 33.5 years and Jin HR et al [92] reported mean age of 37 years in their studies. In present study male predominance in cases of deviated nasal septum was observed. With male to female ratio 1.9: 1. Ratio of 1.8: 1 in Jin HR et al9 and 2.2:1 in Janardhan Rao et al10 studies have been reported. It maybe because of males are the one who responsible person in the family and also try to become get rid of sick things immediately. That is why they come to hospital early for treatment as compared to female who often tend to neglect their health problem. In present study, the most common complaints seen in patients of deviated nasal septum was nasal obstruction (90%), followed by nasal discharge (72%).Least common symptom was nasal bleeding seen in 5% cases.A deviated nasal septum is the most common cause of nasal obstruction. It influences the airflow dynamics of the nasal cavity and improper aeration of paranasal sinuses. Due to airflow changes, compensatory hypertrophy of the nasal mucosa on concave side is often found which lead to bilateral nasal obstruction11. Nasal discharge is also seen in deviated nasal septum patient. As patients with deviated nasal septum may lead to improper aeration of paranasal sinus which causes inflammation of the mucosa of the paranasal sinuses. As mucosal inflammation is the central pathophysiological mechanism that underlies many of the specific and interrelated factors that contribute to congestion, including increased venous engorgement, increased nasal secretions and tissue edema.12Headache is also the most common presenting symptom reported by many studies. The cause of headache is attributed to mal-ventilation of sinuses due to presence of deviation of nasal septum leading to local hypoxia, reduced pH, reduced ciliary beat and thick viscous mucous and increased vulnerability to infection leading to headache. Headache associated with facial pain are treated as “sinus” headache.13Similar findings were also observed by Jareoncharsri et al14, Asruddin et al15, Kolvekar et al16 and Venkatachalam17. In present study severe septal deviation was more frequently associated with sinusitis on same side and was seen in 44% cases.Among moderate septal deviation it was found that sinusitis on the side of septal deviation in 27% cases. There was significantassociation of septal deviation with sinusitis (X2 =11.27, DF = 2, P value<0.05). Lamellar concha bullosa was mostly acceptable as a normal anatomical variation. True and bulbous concha bullosa were caused obstruction and pressure to surrounding the normal airflow, mucociliary activity and drainage and lead to mucosal edema. In present study, sinusitis was determined in 22% of lamellar, in 18% of bulbous and in 15% true concha bullosa cases. There was no significant association of concha bullosa on same side with sinusitis (X2=3.57, DF= 2, P value >0.05). Hatipolgu et al18also found no significant difference between type of concha bullosa and association with sinusitis on same side. Stallman et al19 failed to show a relationship with sinusitis in a study by which concha bullosa was classified according to size. Paradoxical middle turbinate was observed in 25% cases in present study. Agger nasi was seen in 55% cases, haller cell in 11% cases, enlarged ethmoidal bulla in 15% cases were on same side of disease . But there was no significant association between the anatomical variation and sinusitis on same side of disease (X2 = 0.73, DF = 3, P > 0.05). Simliarly there was no significant association between the anatomical variation and sinusitis on opposite side of disease Kim et al20, Lerdlum and Vachiranubhap21, and Stallman et al19 also demonstrated no specific associations underlined the local, systemic, environmental factors or intrinsic mucosal disease in the pathogenesis of rhinosinusitis. Thus the findings were comparable with the present study.
CONCLUSION With reference above mentioned results and discussion we conclude that there was a significant association of septal deviation with the sinusitis on same side while there was not significant concha bullosa and its association with sinusitis on same side. The association of other anatomical variation and sinusitis on same side was not significantly associated.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.