 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 3 - June 2019
Clinico-pathological study of patients of hoarseness of voice in adult of north India region
Madhukar Vashistha*, Neetu Shukla**, Abha Mishra***, Sanjeev Kumar****, Mamta Dwivedi*****
*Assistant Professor, Department of ENT, Rama Medical College, Kanpur, INDIA. **Assistant Professor, Department of ENT, TS Misra Medical College, Lucknow, INDIA. ***Associate Professor, Department of Pathology, TS Misra Medical College, Lucknow, INDIA. ****Associate Professor, Department of ENT, TS Misra Medical College, Lucknow, INDIA. *****Senior Resident, Department of Pathology, KGMU, Lucknow, INDIA. Email:neetushuklaoct@gmail.com
Abstract Background: Voice disorders typically present with hoarseness and hoarseness is one of the commonest symptoms in otolaryngology outpatient clinic and is invariably the earliest manifestation of condition directly or indirectly affecting the voice apparatus. It should be emphasized that hoarseness is not a disease in itself but a symptom of disease or disturbance of larynx or laryngeal innervations. The aim of the study was to analyse various causes and conditions associated with hoarseness of voice. Material and Method: We studied 200 patients with an age range of between 11 to 90 years. All the routine investigations like Hb, BT, CT, TLC, DLC, urine-for albumin and sugar were carried out in all patients. X-ray chest- PA view and X-Ray soft tissue neck- AP and lateral view were done when required. Larynx was examined by flexible fibreoptic laryngoscopy followed by biopsy if suspicious looking area was seen. Results: The majority of patients were male and M: F ratio was 4.26:1 and had a peak age distribution of 31 to 60 years (69%). In this study, level of voice disorders formulated by Koufman was adopted. The commonest occupation was being farmers (18.5%) manual labours (16%), traders (15%), teachers (14.5%) and housewife (11.5%) and majority of patients were level (IV) voice users (32.15%). The commonest etiology of hoarseness of voice was found to be due to inflammation (31%) or infection of upper respiratory system (22.5%) followed by vocal cord nodule (12%), Vocal cord polyp (9%), functional voice disorders (5%), and vocal cord paralysis (5.5%) vocal cord cancer (5.5%) and congenital disorders (3.5%). Conclusion: The most common symptom associated with hoarseness in patient was cough reported in (42) of patients, throat pain (in 38 patients) .and painful swelling in 30 patients and other clinical features were also reported during OPD visit like epigastric pain (9.5%), retrostrnal pain (8.5%), hemoptysis (5.5%), stridor (1.5%), aphonia (1%), aspiration (1%).Proper medical history, complete investigation and management are therefore required to treat the underlying pathology. Keywords: Hoarseness of voice, North India.
INTRODUCTION Voice is the sound produced by vocal cord and uttered by the mouth, which can be heard or measured. The normal voice should possess certain characteristics of pitch, loudness and quality which make clear meaning and elicits an emotional response to ensure a pleasant tonal effect upon the listener.1 Voice disorders typically present with hoarseness and hoarseness is one of the commonest symptoms in otolaryngology outpatient clinic and is invariably the earliest manifestation of condition directly or indirectly affecting the voice apparatus. Hoarseness is defined as abnormal production of sound, perceived as raspiness, breathiness, harshness, vocal tension or lower pitched voice. Any patient with hoarseness of two week duration or longer must visit hospital for entire larynx visualization, particularly the vocal folds. The complaint of hoarseness of long duration may imply serious disease so it should not be ignored. Hoarseness may indicate disease ranging from totally benign condition to the most malignant lesion with or without metastasis. Proper medical history, investigation and management are therefore required to treat the underlying pathology. Hoarseness may be acute or chronic depending on the duration of illness. Acute hoarseness is caused by acute laryngitis, viral infection, smoking, vocal abuse, thyroid surgery, or laryngeal trauma Chronic onset is mainly caused by vocal cord abuse, nodule, polyp, laryngeal papillomatosis, thyroid oesophageal or lung cancer, chronic granulomatous disease like tuberculosis or systemic disease including diabetes mellitus2. MATERIAL AND METHODS This retrospective study was conducted in the department of Otorhinolaryngology, at Rama medical College, Kanpur, one of tertiary centre from May 2017 to December 2018.Demographic data was recorded in terms of age, sex and the site of involvements with pattern of clinical and pathological presentation from case sheet collected form Medical record department of hospital. Diagnosis was mainly made by indirect laryngoscopy and flexible nasopharyngeal video laryngoscopy, CT scan (axial, coronal image) and histopathological examination3.. The detailed history, clinical profile, routine investigations (CBC, blood sugar level, Urine examination) and radiological investigations (X-Ray chest PA view, X-Ray soft tissue neck AP/Lateral view) and indirect larygoscopy report were also analysed and tabulated. Histopathological examination of suspected benign and malignant cases was done in all suspected cases4. Inclusion Criteria- All cases of hoarseness with duration of two weeks or more than two weeks attended otolaryngology OPD during January 2016 – December 18 were included Exclusion Criteria- Patients of hoarseness with less than two weeks duration of hoarseness were not included.
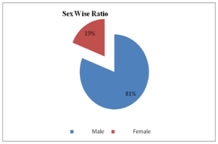
OBSERVATION AND RESULT Table 1: Sex Wise Distribution of Patients
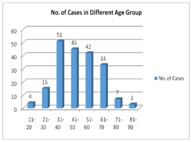
Table 2:Age Wise Distribution of Hoarseness of voice
Table 3: Occupation Wise Distribution of Hoarseness of voice
Table 4: Duration of Hoarseness of Voice in Patients
Table 5: Various causes of Hoarseness of Voice with Etiology
Table 6: Commonest Associated Symptoms /Signs in Hoarseness
OBSERVATION Present study included 200 patients with an age range of between 11 to 90 years The majority of patients were male with M: F ratio of 4.26:1 and had a peak age distribution of 31 to 60 years (69%). In this study level of voice disorders formulated by Koufman were adopted and these four levels are selected by Koufman et la for approaching voice disorders .A Koufman criterion has been grouped as follow…..
The commonest occupation was being farmers (18.5%) manual labours (16%), traders (15%) teachers (14.5%) and housewife (11.5%). Majority of patients were level (IV) voice users (32.15%). Occupation appears to predispose one to the level of voice use or vocal environment that increases the chance of getting a voice disorder. The diagnosis of the commonest condition causing horsiness of voice was due to chronic nonspecific laryngitis (31%) while laryngitis accounting in 22.5% cases. The most common symptom was cough reported in 42 of patients, throat pain in 38 patients and painful swelling in 30 patients and other features are epigastric pain, retrostrnal pain, hemoptysis, stridor, aphonia, aspiration. Banjara et al (2011) mentioned age range to be 11-78 years in their study and majority of patients presented in 4th and 6th decades of life (22.31% each).This is in accordance with our study in which age of presentation ranged from 11- 90 years with maximum cases in third and fourth decade of life, which is the period of most active life when man indulges in vocal abuse. Banjara et al (2011) also observed male preponderance with male: female ratio as 1.89:1 in their study. This can be attributed to the fact that males indulge more in smoking, alcoholism, pollutant exposure and misuse of voice. In contrast, Brodnitz (1963) has documented an almost equal number for both sexes with a slight preponderance of males but the individual conditions exhibited marked difference. In our study, besides change in voice other associated features were cough (42), throat pain (38), painfull swelling (30) dysphagia (12) and while Ghulam et al reported hoarseness of voice (100%) to the most common presenting feature associated with dysphagia (63%),dyspnoea (36.95%) and pain throat (48.91%). Banjara et al( 2011) reported change in voice (95.61%)as most common complaint associated with dysphagia (16%),foreign body sensation (16%)and vocal fatigue(10%).In the present study, chronic non specific laryngitis (31%%) was the most common pathology followed by specific laryngitis (22.5%%) vocal cord nodule (12%), vocal cord polyp (9%),contact ulcer (6%), vocal cord palsy, vocal cord cancer (5.5% each) functional voice disorder (5%) and congenital laryngeal web (3.5%). Banjara et al (2011) mentioned functional lesions (16.33%) to be most common etiology followed by vocal nodule (11.95%), vocal palsy (11.16%), cancer and chronic laryngitis (9.56% each). The duration of hoarseness of voice since onset of the symptoms and the first treatment given either at primary, secondary or even at referral unit ranged from 14 days - 52 years. In our study most of the patients (28%) suffered from hoarseness of voice for more than 1year before seeking medical advice. 21.5% cases complaint of hoarseness within 2- 4 weeks 19.5% cases visited after 5-12 weeks and 16% cases came after 4-6 months.. Banjara et al found that most of the patients (61%) having complain of hoarseness for 3 months & 21% for duration of 3 to 6 months. Smoking habits along with tobacco chewing is found to be most important predisposing factors for development of hoarseness.
DISCUSSION Most voice disorders are multifactorial in etiology and are related to irritation from possible reflux, allergies, smoking, inadequate hydration, vocal abuse, and/or chronic vocal hyper function. Voice therapy is often successful in the treatment of functional and organic vocal disturbances6. The only entity causing hoarseness that can be treated pharmacologically is chronic laryngitis associated with gastro-oesophageal reflux, which responds to treatment of the reflux disorder7. Indications for the use of antibiotics and/or antihistamine decongestants in patients with hoarseness are common when the patient has concomitant allergic rhinitis or bacterial laryngitis and/ or pharyngities, which may be causing or complicating the patient’s hoarseness. Surgery on the vocal cords is indicated to treat tumour and inadequate vocal cord closure. Microlaryngealsurgery is a common and safe otolaryngological surgery. Microlaryngoscopy is helpful in taking biopsy along with determining the extent of the lesion properly which is necessary for staging and subsequent treatment of the vocal cord cancer .In Indian scenario upper aero- digestive tract malignancy is more common and in laryngeal growth supraglottic being the commonest and carcinoma larynx is common in 5th and 6th decades of life 9.In case of nodules of vocal cord polyps, hoarseness was explained by the fact that lesions involving the free margins of the cords inevitably disrupt the vibratory function of phonation.
CONCLUSION Voice disorders have great impact on any individual’s personal and professional life. Proper history taking, proper diagnosis & management of hoarseness can be a challenge to treating doctor. Direct Laryngoscopy and Fiberoptic Flexible Endoscopy (FOFE) proved to be useful methods in detecting various causes of hoarseness. Biopsy should always be taken from any growth or suspicious area for the confirmation of diagnosis so the proper management can be given at earliest. Management of hoarseness can be a primary issue for the physician. Treatment is individualized depending on the diagnosis and individual needs of the patient. Voice therapy, vocal cord surgery, and drug therapy for appropriate groups of patients with hoarseness are well documented as effective by the available evidence. Laryngeal examination, like laryngoscopy (indirect, flexible and rigid) and Microlaryngoscopy have established diagnostic and therapeutic application so the standard treatment of choice in all types of benign tumours of the larynx should consist of a triad of approach by Microlaryngealsurgery (with or without laser),voice rest and vocal rehabilitation.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.