EVALUATION OF INFERIOR TURBINATE HYPERTROPHY IN PATIENTS WITH DEVIATED NASAL SEPTUM
- A HOSPITAL-BASED STUDY
RAIES AHMAD BEGH1, ADITIYA SARAF2*
Department of ENT and Head and Neck Surgery, SMGS Hospital, Government Medical College, Jammu, Jammu and Kashmir, INDIA.
Abstract Aims and Objectives: to evaluate inferior turbinate hypertrophy in patients with deviated nasal septum. Material and Methods: The present study was conducted on 50 patients attending ENT OPD in SMGS Hospital, GMC Jammu during a period between January 2018 to February 2019. A total of 50 patients within age group of 18-50 years with sino nasal complaints were analysed in our study and were subjected to NCCT nose and paranasal sinuses- axial and coronal cuts. Three measurements were done to document the width of the ITH: (a) total turbinate width (b) medial mucosa width (c) bone width. Nasal septal deviation was classified based on relation of nasal septum with inferior turbinate: Degree I- deviation did not reach the inferior turbinate, Degree II- deviation reached the inferior turbinate, Degree III- deviation reached the lateral wall and compressed inferior turbinate. Patients with Degree I DNS were kept in Group A, patients with Degree II in Group B and patients with Degree III in Group C. Results: The average width values (in mm) of medial mucosa, bone and total turbinate in Group A were found to be 3.21, 0.95 and 5.33 respectively. The average width values (in mm) of medial mucosa, bone and total turbinate in Group B were found to be 4.99, 1.43 and 9.93 respectively. The average width values (in mm) of medial mucosa, bone and total turbinate in Group C were found to be 5.45, 1.77 and 9.97 respectively. Conclusion: In our study, there was varying amount of mucosal hypertrophy of inferior turbinate in different degrees of deviated nasal septum.
Keywords: turbinate, hypertrophy, septum, deviation
INTRODUCTION
The nasal septum develops from the frontonasal process. Initially, it is entirely cartilaginous and together with the triangular cartilages forms a cartilaginous structure that supports the nose from the crista galli to the lower third of the nose. The cephalic part of the septum ossifies from the perpendicular plate of the ethmoidal bone. The vomer develops in the tissues covering the postero-inferior part of septal cartilage as two bony plates with the cartilage between. The perpendicular plate forms the cephalic part of skeleton of septum, the vomer postero-caudal part and quadrilateral cartilage the anterior part.1
Nasal turbinates are bony projections from lateral nasal walls covered with mucosa assisting in warming, filtering and moisturizing the inhaled air.2The turbinates exist as three and sometimes four, bilateral extensions from the lateral wall of nasal cavity. The anterior aspects of the middle and inferior turbinate project into the primary airflow pattern observed during inspiration and expiration. At the inspiration, upto two-thirds of upper airway resistance is produced by the anterior tip of inferior turbinate in the region of the internal nasal valve. Of the three turbinates, inferior turbinate is most susceptible to enlargement. Enlargement of the erectile mucosa of the inferior turbinate significantly increases nasal airway resistance.3Though the term hypertrophy implies as the enlargement of an organ or tissue due to an increase in the size of its cells; herein the term turbinate hypertrophy is widely accepted as increased thickness of soft tissue and/or bone components.2The nasal septum divides nasal cavity into the left and right halves both anatomically and physiologically. It is an accepted fact that some amount of deviation of nasal septum is common and having a perfectly straight septum is a rarity. Various reasons have been attributed to the occurrence of deviated nasal septum including racial factors, birth moulding of septum during parturition trauma and developmental deformities of septum. Deviated nasal septum may cause nasal obstruction and symptoms of rhinosinusitis.4The aim of our present study was to evaluate inferior turbinate hypertrophy in patients with deviated nasal septum.
MATERIAL AND METHODS
The present study was conducted on 50 patients attending ENT OPD in SMGS Hospital, GMC Jammu during a period between January 2018 to February 2019. A total of 50 patients within age group of 18-50 years with sino nasal complaints were analysed in our study and were subjected to NCCT nose and paranasal sinuses- axial and coronal cuts. Scans were reviewed for any nasal cavity/ paranasal sinus abnormality, with emphasis on presence of inferior turbinate hypertrophy and deviated septum. Exclusion criteria of our study were patients with septal hematoma, septal abscess, sino-nasal malignancies, sino-nasal polyposis and age below 18 years. All patients were subjected to relevant clinical history and anterior rhinoscopy. Three measurements were done to document the width of the ITH: (a) total turbinate width measured by maximum transverse width of the pendulous portion of inferior turbinate inclusive of soft tissue and bone. (b) medial mucosa width was measured as transverse thickness at the point of maximal soft tissue thickness along the medial aspect of inferior turbinate. (c) bone width was represented by maximum transverse width of inferior conchal bone. [2]These measurements were taken separately at the maximum hypertrophied portion of inferior turbinate at a place perpendicular to the mucosal surface with the aid of a cursor on the screen of CT console. Nasal septal deviation was classified based on relation of nasal septum with inferior turbinate: Degree I- deviation did not reach the inferior turbinate, Degree II- deviation reached the inferior turbinate, Degree III- deviation reached the lateral wall and compressed inferior turbinate. Patients with Degree I DNS were kept in Group A, patients with Degree II in Group B and patients with Degree III in Group C.
RESULTS
Majority of patients in our study belonged to age group of 31-40 years, with mean age of presentation being 35.4 years(Figure 1).
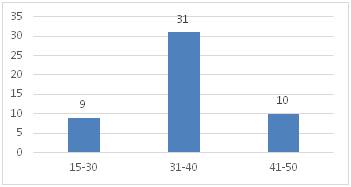
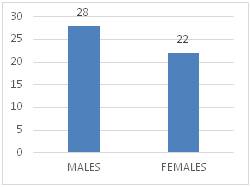
Figure 1 Figure 2
In figure 2 , Out of 50 patients, 28 were males and 22 were females. In figure 3, the major presenting complaint was nasal obstruction(100%), followed by nasal discharge(64%) and epistaxis(10%).
In figure 4, Out of 50 patients with sino-nasal complaints in our study, deviated nasal septum was present in 45 patients, which were assigned into Group A , B and C , as per the degree of deviation. Group A comprised of 28 patients, Group B comprised of 11 patients and Group C comprised of 6 patients.
In Table, The average width values (in mm) of medial mucosa, bone and total turbinate in Group A were found to be 3.21, 0.95 and 5.33 respectively. The average width values (in mm) of medial mucosa, bone and total turbinate in Group B were found to be 4.99, 1.43 and 9.93 respectively. The average width values (in mm) of medial mucosa, bone and total turbinate in Group C were found to be 5.45, 1.77 and 9.97 respectively.
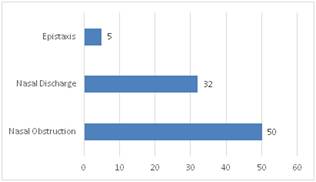
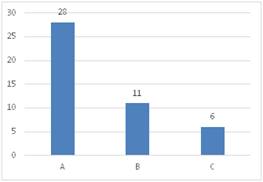
Figure 3 Figure 4
Table 1:
Measurements of Contralateral ITH |
Group A |
Group B |
Group C |
Medial mucosa |
3.21 |
4.99 |
5.45 |
Bony Width |
0.95 |
1.43 |
1.77 |
Total Turbinate width |
5.33 |
9.93 |
9.97 |
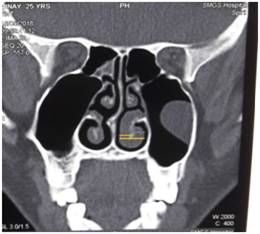

Figure 5 Figure 6
Figure 5: Upper line showing medial mucosa hypertrophy and lower line showing total turbinate width
Figure 6: Line showing bony width
DISCUSSION
Septal deviation with turbinate hypertrophy is considered the main structural cause of chronic nasal obstruction. In patients with septal deviation, compensatory inferior turbinate hypertrophy is often found in the contralateral side to the major septal deviation. Majority of patients in our study belonged to age group of 31-40 years, with mean age of presentation being 35.4 years. Out of 50 patients, 28 were males and 22 were females. The major presenting complaint was nasal obstruction(100%), followed by nasal discharge(64%) and epistaxis(10%).Out of 50 patients with sino-nasal complaints in our study, deviated nasal septum was present in 45 patients, which were assigned into Group A , B and C , as per the degree of deviation. Group A comprised of 28 patients, Group B comprised of 11 patients and Group C comprised of 6 patients. The average width values (in mm) of medial mucosa, bone and total turbinate in Group A were found to be 3.21, 0.95 and 5.33 respectively. The average width values (in mm) of medial mucosa, bone and total turbinate in Group B were found to be 4.99, 1.43 and 9.93 respectively. The average width values (in mm) of medial mucosa, bone and total turbinate in Group C were found to be 5.45, 1.77 and 9.97 respectively. Thus in our study, medial mucosa undergoes more hypertrophy than bone width of inferior turbinate. Berger et al., found that inferior turbinate hypertrophy was caused by conchal bone hypertrophy rather than medial and lateral mucosal hypertrophy. 6.Egeli et al. found that compensatory turbinate hypertrophy was due to both conchal bone enlargement and medial and lateral mucosal hypertrophy.3 Orhan et al. used CT to prove that compensatory hypertrophy of inferior turbinate in patients with nasal septum deviation is caused not only by mucosal hypertrophy but also by inferior turbinate hypertrophy itself.7Sahu et al., in their study concluded that degree of compensatory hypertrophy of inferior turbinate is increased in direct proportion with the severity of the DNS. The medial mucosa undergoes maximum hypertrophy as compared to the bone width.2
CONCLUSION
Among all three nasal concha, inferior turbinate is most susceptible for enlargement. Unilateral turbinate enlargement is seen with contralateral septal deviation to prevent the crusting and drying effects by excess airflow. In our study, there was varying amount of mucosal hypertrophy of inferior turbinate in different degrees of deviated nasal septum.
REFERENCES
- Scott-Brown’s Otorhinolaryngology, Head and Neck Surgery, 7 /e. Volume 2;Part 13: Chapter 123.
- Sahu N, Mohapatra S, Rath S, Padhy R. Computed Tomographic Evaluation of Inferior Turbinate Hypertrophy In Adult Indo-Dravidian Patients With Deviated Nasal Septum. Asian J Pharm Clin Res.2017;Vol 10:342-344.
- Egeli E, Demirci L, Yazycy B, Harputluoglu U. Evaluation of the inferior turbinate in patients with deviated nasal septum by using computed tomography. Laryngoscope. 2004;114(1):113-7.
- Arora M, Ali S, Choudhary AK, Suchit K, Bansal C. Correlation between Deviated Nasal Septum and Sinusitis: A Clinical and Histopathological Study. Int J Sci Stud. 2016;4(1):21-24.
- T.D.A. Vidigal, F.L.M. Haddad, L.C. Gregorio, D. Poyares, S. Tufik, L.R.A. Bittencourt. Subjective, anatomical and functional nasal evaluation of patients with obstructive sleep apnoea syndrome. Sleep and Breathing.2013;17(1):427-433.
- Berger G, Hammel I, Berger R, Avraham S, Ophir D. Histopathology of the inferior turbinate with compensatory hypertrophy in patients with deviated nasal septum. Laryngoscope 2000;110(12):2100-5.
- Orhan I, Aydin S, Ormeci T, Yilmaz F. A radiological analysis of inferior turbinate in patients with deviated nasal septum by using computed tomography. Am J Rhinol Allergy.2014;28(1):68-72.
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.