 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 2 - August 2019
Rodny Alex Thomas*, Rajarajeswari N**, Mary Kurien***, CM Rajakumar#, Meenu Khurana Cherian##
*Specialist ENT, Asian Medical centre, QATAR. *Assistant Professor, **Professor and HOD, Department of ENT, Pondicherry Institute of Medical Sciences, Puducherry, INDIA. #Private Practitioner, Otorhinolaryngology, Chennai, INDIA. ##Specialist ENT, Thumbay Hospital, Ajman, UAE. Email: rajisampathporal@gmail.com
Abstract Background: Tonsillectomy is done for various indications, the commonest being recurrent/chronic tonsillitis and tonsils presenting with obstructive symptoms. Studies have proved that swab culture from the tonsillar surface is not a true indicator of the organism present in the core. This study was done to compare the organisms that cause recurrent/chronic tonsillitis and those that cause enlargement of the tonsils leading to obstructive symptoms. Methods: Fifty patients undergoing tonsillectomy were included in the study. Among them, the indication for tonsillectomy was chronic tonsillitis and hypertrophied tonsillitis with obstructive symptoms, 25 patients being in each group. Following tonsillectomy, core tonsillar tissue was sent for culture and sensitivity. Results: In patients with recurrent or chronic tonsillitis, tonsil core was positive for culture in 100%, Staphylococcus aureus being the commonest pathogen (52.0%), followed by Hemophilus influenza (32%). In those who presented with obstructive symptoms tonsil core did not grow any organism in 88% of the patients, the rest 12% being Streptococcus pyogenes and Streptococcus pneumoniae. Conclusion: In patients with chronic / recurrent tonsillitis, the tonsil core was positive for culture in all, unlike those with primarily obstructive symptoms with hypertrophied tonsils, which did not grow any organism in majority of them. Trial of appropriate antibiotic therapy could be instituted in patients with recurrent/chronic tonsillitis whereas in those with obstructive symptoms administration of antibiotic therapy would prove to be of little or no use. Besides in the former group, presence of intra-tonsillar infection suggests need for perioperative antibiotic therapy. Key Word: Tonsillitis, Hypertrophied tonsils, Coreculture, Antibiotic sensitivity.
INTRODUCTION Tonsils are immunologically more active in the first years of life. During aging, whereas lymphoid tissue regresses, sub epithelial tissue changes into fibrotic tissue and crypts alter into cavities filled with keratin. In case of infection, bacteria that inhabit the crypts spread into the tonsil and leave their toxins and other products in it, eventually leading to polymorphpo nuclear leukocyte infiltration, swelling, necrosis and surface ulceration in tonsils. Consequently, after acute infection, bacteria may inoculate into the core1. These infections are highly frequent especially in childhood. Although antibiotic therapy may be sufficient in the treatment of acute tonsillitis, tonsillectomy remains the treatment of choice in the management of recurrent and chronic tonsillitis2. Inappropriate antibiotic therapy against the pathogen in deep tissue or inadequate antibiotic levels in the tonsillar tissue leads to the continuation of the infection and the re-inoculation of thesurface3. It has been claimed that the results of the cultures taken from tonsillar surfaces may not always show the real pathogen4. Bacterial agents such as Group A Beta hemolytic streptococci, staphylococcus aureus, hemophilus influenza, streptococcus pneumonia, Corynebacterium diptheriae and Neisseria gonorrhea are the main causes of tonsillitis5. This microorganism is different from other agents causing tonsillitis for the following reasons: it may lead to Rheumatic fever and Acute Glomerulonephritis, its treatment is easy and it is still sensitive to penicillin. Medical therapy is the first step in the management of recurrent tonsillitis and surgical treatment is reserved for cases in which medical treatment fails. Recurrent tonsillitis is defined as infection of the tonsils associated with sorethroat, fever and tonsillar enlargement with more than six such episodes lasting for 3- 4 days in the 1st year, more than three episodes per year for two or more years6.Chronic tonsillitis is defined as infection of the tonsils that’s unresponsive to medical therapy associated with halitosis, tender cervical adenitis and persistent sore throat: seven or more episodes of sore throat in the preceding year who were treated with antibiotics, five or more episodes of sore throat in the preceding two years and three or more episodes in each of the three preceding years. Tonsillitis with obstructive symptoms is defined as episodes of tonsillitis that present with the features of Obstructive sleep apnoea which is defined as 30 or more episodes of cessation of airflow at the nostrils and mouth for at least 10 seconds occurring during a seven hour sleep period. It is further classified into
There is associated mouth breathing and snoring. Many micro-organisms can induce inflammation in Waldeyer's ring. These include aerobic as well as anaerobic bacteria, viruses, and chlamydia, yeasts, parasites, and rickettsia. Some of the organisms are part of the normal oropharyngeal flora that can become virulent, and some are external pathogens. Because the oropharynx is colonized by many organisms, most infections of the ring are polymicrobial. Because of the polymicrobial nature of most infections in and around Waldeyer's ring, it is often difficult to interpret data derived from clinical samples obtained from mucous surfaces and then differentiate between organisms that are colonizers and those that are invaders. However, an avirulent colonizer can become a virulent pathogen under certain conditions, especially in the chronic stage of the disease 7.Enlargement of the chronically inflamed tonsil is due to the presence of a large number of lymphocytes, plus an increased amount of connective tissue, neutrophils, and occasional keratin cysts. Infrequently, enlargement is due to chronic abscesses. After an acute infection, the bacteria may be harboured within the core, leading to chronic infection. Determination of the core bacteriology may be important for several reasons. First, these bacteria may be the organisms that lead to the changes listed above. Secondly, the failure to eradicate the organisms in the core, whether it is from inappropriate antibiotic choice or from insufficient antibiotic penetration into the core, will allow either persistence of core infection or re-inoculation of the initially sterilized surface. Lastly, as suggested by several authors, bacteria harboured in the core may exert a protective effect on other pathogens, such as the protection of group A β-haemolytic streptococci from Penicillin by the β-lactamase production of Staphylococci8. Though diagnosis of chronic tonsillitis is mainly by history and clinical examination, throat swab as a main investigation to confirm this is still used in most developing countries to confirm this. It is also well accepted that effective treatment of chronic tonsillitis depends on knowledge of the infecting organism. Superficial tonsil swabs are often used as a guide in the selection of this therapy in tonsillitis. However several studies indicate a marked discrepancy in the surface and core pathogen flora9,10,11,,14, and raise the question whether surface cultures can accurately predict the presence of β-lactamase producing organisms or other pathogens in the recurrently infected tonsil12,13. In a prospective study of 40 patients clinically diagnosed to have chronic tonsillitis undergoing tonsillectomy the reliability of the throat surface swab was assessed and validated with the reference (gold) standard of tonsil core culture. The results showed that routine culture of the throat by surface swab in the accurate diagnosis of bacterial flora in chronic tonsillitis is neither reliable nor valid.14. There has been paucity of data regarding the microbiology of tonsil core in patients with chronic or recurrent tonsillitis and hypertrophied tonsils with obstructive symptoms only. Hence this study was undertaken.
MATERIALS AND METHOD This study was carried out in the Department of Otorhinolaryngology, Pondicherry Institute of Medical Sciences, Puducherry over a period of 18 months, following Institutional Research and Ethical Committee clearance in accordance with ICMR national ethical guidelines for biomedical research. Fifty patients of all age groups and both the sexes admitted for tonsillectomy were selected for the study. Type Of Study: A prospective study. Inclusion Criteria All patients admitted to the hospital wards in PIMS for tonsillectomy for
Exclusion Criteria
Method of collection of data: Following this a detailed history and examination investigations including haemoglobin, bleeding time, clotting time and HIV serology were done for all patients prior to surgery. Method of collection of culture specimens: All patients underwent tonsillectomy by dissection and snare method. Excised tonsils were placed in normal saline and tissue was taken from the core using aseptic precautions incising the tonsil with a sterile blade and with another sterile blade only the core was extracted in a wedge shaped manner. Culture was done in aerobic media for a period of 24 – 48 hours.
RESULTS In this study of 50 patients, there were 28 male and 22 female patients. Patients who had recurrent/chronic tonsillitis were categorized in Group 1. Patients who presented with obstructive symptoms were categorized in Group 2. There were 25 patients in each group. The age distribution in each group is given in table 1. The comparative age between the two groups were almost similar. Table 1: Age Distribution
Symptoms in patients in Group 1 ranged between odynophagia (80%), sore throat or a burning sensation in the throat (52%), feeling of swelling in the throat (32%) and foreign body sensation (8%). Of the 25 patients that complained of obstructive symptoms all of them complained of swelling and dysphagia, mouth breathing was observed in (44%) and a foreign body sensation observed in (12%) of the patients that were studied (figure 1).
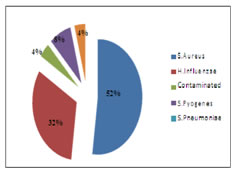
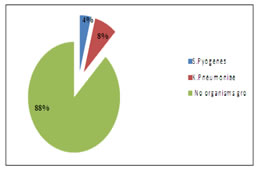
Figure 1: Oropharynx: Signs and Symptoms Figure 2: Tonsillar Hypertrophy In patients who did not present with obstructive symptoms, the grade of tonsillar hypertrophy was Grade 1 (60%), Grade 2 (32%) and Grade 3 (8%). Those that did present with obstructive symptoms the grade of tonsillar hypertrophy was Grade 3 being (48%) and Grade 4 being (52%) (Figure2). The most common organism cultured from the core in patients with recurrent/chronic tonsillitis (where culture was positive in all) was S. aureus (52%), H. influenzae (32%), S. pyogenes (8%), K. pneumoniae (4%), with one sample being contaminated. In contrast to the organisms grown in patients who presented with recurrent/chronic tonsillitis, the patients who presented with obstructive symptoms did not grow any organism from the tonsillar core on culture in 88% of the cases. The organisms that did grow were K. pneumoniae (8%) and S. pyogenes (4%). (Table 2, Figures 3 and4).
Table 2: Organisms Grown
Group 1 Group 2
DISCUSSION The pathogenesis of infectious / inflammatory disease in the tonsils most likely has its basis in their anatomic location and their inherent function as organ of immunity, processing infectious material, and other antigens and then becoming, paradoxically, a focus of infection/inflammation. Several pieces of direct and indirect evidence indicate that the palatine tonsils are continuously engaged in local immune responses to microorganisms. If the tonsillar lymphocytes became overwhelmed with this persistent stimulation they may be unable to respond to other antigens; the immunological response, particularly in recurrent tonsillitis, may then be impaired.15 Tonsillar hypertrophy is the enlargement of the tonsils, but without the history of inflammation. Hyperplasia itself is not a disease, but only a result of increased immunologic activity. It does not necessary be due to inflammation or tonsillitis.16,17 As a norm, all cases that presented with recurrent / chronic tonsillitis, a throat swab was the first line of management. Normal bacterial flora present in the oral cavity and oropharynx were cultured in most cases and antibiotic therapy was instituted based on the results obtained from the cultures grown by the throat swab. Several studies have disapproved this theory.14,18 The most common organisms that were found in the tonsillar core were Group A beta-hemolytic Streptococcus, S. aureus, H. influenzae and S.pneumoniae.18,19 This correlates to our study in that the most common organisms isolated from the core in cases of recurrent / chronic tonsillitis were S. aureus and H. influenzae. In our study it was found out that patients that presented with hypertrophied tonsils with obstructive symptoms, no organisms were grown in 88% of the patients, the remaining 12% of the patients grew K. pneumoniae (8%) and S. pyogenes (4%). Quantitative bacteriology of tonsils removed from children with tonsillitis hypertrophy and recurrent tonsillitis with and without hypertrophy revealed that aerobic and anaerobic bacterial species were present in all tonsils. The predominant aerobic and facultative organisms were Haemophilus influenzae, Neisseria species and Staphylococcus aureus, and predominant anaerobic bacteria were Fusobacterium species, Bacteroides species, and Prevotellamelaninogenica. A higher concentration of S. aureus and H. influenzae was found in hypertrophic tonsils as compared to recurrent tonsillitis. These findings suggest the presence of an increased bacterial load and support an etiologic role for H. influenzae and S. aureus in hypertrophic tonsils with and without the presence or absence of core pathogens in 32% of the study group. The core only was pathogenic in 12% and the group which isolated a different pathogen on the surface and core was 20%.8 On the contrary our study showed that the core tissue of all those with chronic tonsillitis grew micro-organisms while those with hypertophic tonsils only 12% grew micro-organisms. The role of anaerobic bacteria in tonsillitis is hard to elucidate because these organisms are normally prevalent on the surface of the tonsils and pharynx as well as in the core of the tonsils, making cultures taken directly from these areas difficult to interpret. Many of the Gram –ve anaerobic bacilli that are isolated from the tonsillar core can produce the enzyme beta–lactamase. Beta lactamase producing strains of Bacteroidesfragilis group, Fusobacterium spp., Haemophilus influenzae and Staphylococcus aureus were isolated from the tonsils of 73% - 80% of children with GABHS recurrent tonsillitis and 40% of children of non GABHS tonsillitis.20 The production of beta – lactamase has important implications for antimicrobial therapy. Limitations: Anaerobic culture was not included due to financial constraints.
CONCLUSION In our comparative study of microbiology of tonsillar core in chronic tonsillitis and in hypertrophied tonsils with obstructive symptoms revealed that the tonsil core tissue grew infective organism in all specimens (100%) in the former group and only in 12% in the latter group. This has clinical significance in the use of prophylactic antibiotics, a highly controversial issue in the perioperative period of tonsillectomy. Broad spectrum antibiotics can be given for those in whom tonsillectomy done for tonsillitis. In those in whom surgery is done for hypertrophied tonsils with obstructive symptoms, antibiotics can be reserved if core tonsil smear is positive tobe followed up on culture. This is the first report of its kind.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.