 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 2 - August 2019
Evaluation of clinical profile of patients with laryngo- tracheal narrowing in a tertiary care centre
Shafaque Warsi1*, Arun Dehadaray2, Maitri Kaushik3, Prasun Mishra4, Viraj Gaikwad5
1Senior Resident, 2Professor, 3Professor and HOD, 4Associate Professor, 5Junior Resident, Department of ENT and Head and Neck surgery, Bharati Vidyapeeth To Be Deemed University Medical College and Hospital Dhankawdi Satara Road-411043, Maharashtra, INDIA. Email: dr.shafaquewarsi@gmail.com
Abstract Background: Laryngo-tracheal narrowing refers to partial or complete narrowing of the endolarynx or trachea. It can be a life threatening condition and has varied etiology. Objectives: To find out the etiology, clinical presentation and severity and site of narrowing in patients with laryngo-tracheal narrowing. Patients And Methods: Observational(cross sectional) study, included 50 patients coming/referred to ENT OPD with complaints of respiratory distress due to various laryngo-tracheal pathologies. Detailed ENT history and examination was carried out. Patients underwent Videolaryngoscopy, X ray neck (AP/Lateral), CT/MRI neck and thorax (plain/contrast) and Direct laryngoscopy. Patients were educated and explained about the procedures. Written informed consent was taken prior to procedures as per attached proforma. Videolaryngoscopy was not done for patients<5 years of age. Results: Among 50 cases of laryngo-treacheal narrowing, majority presented with malignancy (44%) as the most common etiology, followed by post intubation trauma(32%).The commonest clinical presentation is difficulty in breathing followed by change in voice. Equal number of patients had supraglottis and subglottis as the most common site of narrowing. Congenital etiologies were identified by DL scopy and HRCT. Inflammatory conditions were best identified with HRCT. Video laryngoscopy was the best investigation to diagnose neoplastic and neurological conditions. For traumatic pathologies, both DL scopy and HRCT were equally efficient. VLscopy was helpful in external trauma cases. X ray had little significance. Conclusion: The most common etiology for laryngo-tracheal narrowing is neoplasm followed by post intubation trauma. Most common clinical presentation with laryngo-tracheal narrowing is difficulty in breathing, followed by change in voice, and difficulty in swallowing. For laryngo-tracheal narrowing cases with tracheal and congenital etiology like subglottic stenosis, direct laryngoscopy with 0 degree endoscope, is the best modality of investigation. Key Word: Laryngo-tracheal narrowing, Direct laryngoscopy, High resolution computed tomography, Videolaryngoscopy.
INTRODUCTION Laryngo-tracheal narrowing refers to partial or complete narrowing of the endolarynx or trachea. It can be a life-threatening condition and has varied etiology. It is a heterogenous group of conditions leading to severe respiratory distress in a wide range of population1. The term encompasses luminal compromise at the level of larynx or trachea and may be present in more than one anatomical location1. Laryngo-tracheal narrowing is generally described in terms of its structural characteristics, defined in anatomic terms (percent of narrowing, distance from vocal folds, overall length)2.Assessment of severity of narrowing is essential and relevant to management decisions. Laryngeal narrowing may affect supraglottis, glottis and sub glottis. Sub glottis has a higher chance of getting narrow due to its inherent anatomical feature of being a complete circular cartilage, being narrowest in neonates and lined by respiratory epithelium. The normal lumen at subglottis is 4.55.5 mm in newborns, 43 mm in adults males and 36 mm in adult females3. A size of less than 4.0 mm in a full term infant and less than 3.5 mm in premature infants is considered as stenotic. In recent times the incidence of laryngo-tracheal narrowing has become more common for reasons like increasingly prolonged endotracheal intubation for mechanical ventilation, increased incidence of patients coming out of intensive and critical care4. However congenital and infective causes are also not uncommon5. In last few decades, the causes have changed whereby external trauma and infection has been supplemented by iatrogenic trauma from intubation and tracheostomy. Also, narrowing due to external pressure on neck and thorax can now be detected by advanced imaging techniques. Approximately, 15% of patients who are intubated for more than 10 days develop some form of laryngo-tracheal narrowing5. About 90% of acquired subglottic narrowing in infants and children is due to endotracheal intubation. Post intubation tracheal narrowing is less common but not rare. The cuff pressure of endotracheal and tracheostomy tube may play a role in such tracheal narrowing3. Considering the severity of this condition and increase in its incidence in recent times, it is essential to determine the common and precise etiology of laryngotracheal narrowing. Besides, the data of etiology of such condition is very sparse and less amongst Indian population. Present study was planned with the purpose to study and understand the heterogenous etiology and severity of laryngo-tracheal narrowing by means of clinical history, radiological and airway endoscopic evaluation. MATERIALS AND METHODSThis observational(cross sectional) study was conducted in Bharati hospital, Pune from September 2015 to August 2017.It included patients coming/referred to ENT OPD of B.V.D.U.M.C. (a tertiary care teaching hospital) with complaints of respiratory distress due to various laryngo-tracheal pathologies. All patients visiting Bharati Hospital and Research Centre with complaints of respiratory distress of nonpulmonary origin.50 patients with various laryngo-tracheal pathology were evaluated. Inclusion criteria: All cases of acute respiratory distress suspected of laryngo-tracheal pathology. All chronic cases with complaints of breathing difficulties of non-pulmonary origin. All cases of laryngo-tracheal oedema not responding to medical line of management. Exclusion criteria: Un co-operative patients. Non-laryngo-tracheal respiratory distress. Cases where procedure is not possible due to marked trismus, spinal injury. Unconscious patient with altered sensorium. A detailed ENT history taking and examination was carried out for all patients. Cases with laryngo-tracheal narrowing detected on ENT examination were taken for this study. The patients underwent Videolaryngoscopy, X ray neck (AP/Lateral), CT/MRI neck and thorax (plain/contrast) and Direct laryngoscopy. All examinations were performed as per the requirement. Patients were educated and explained about the procedures. Written informed consent was taken prior to procedures as per attached proforma. Videolaryngoscopy was not done for patients<5 years of age The information was collected using a structured proforma and data was entered in excel sheet. Collected data was filled in Microsoft Excel Sheet and analysed using appropriate statistical package. The analysis of data in this study was done using Microsoft Excel and SPSS.
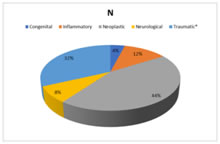
RESULTMost common etiology of laryngo-tracheal narrowing observed in present study was neoplasm (44%) followed by post-intubation trauma (28%). Other etiologies were inflammatory (12%), neurological (8%), congenital (4%) and external trauma (4%) Graph 1: Distribution of subjects based on Etiology of Laryngo-Tracheal Narrowing2 cases of external trauma and 14 cases of Post-Intubation Site of narrowing was divided into two categories: Laryngeal and Tracheal Laryngeal was further subdivided into: supraglottic, glottic, sub glottic. Out of total 50 cases with laryngeal narrowing, most common sites were supraglottic (32%) and subglottic (32%) with 16 cases each while glottic narrowing was seen in 12 cases(24%). Tracheal narrowing was seen in 6 cases (12%). Table 2: Distribution of cases based on site of narrowing
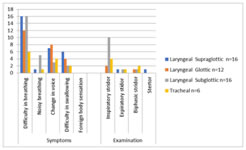
Out of total 16 supraglottic narrowing cases, most common presenting symptom was difficulty in breathing16, followed by change in voice7, and difficulty in swallowing6 . On examination, one patient had expiratory stridor, 1 had stertor. Out of total 12 glottic narrowing cases, most common presenting symptom was difficulty in breathing12, followed by change in voice8 and difficulty in swallowing4. On examination 2 patients had inspiratory stridor 1 had biphasic stridor. Out of total 16 subglottic narrowing cases, most common presenting symptom was difficulty in breathing16, followed by noisy breathing5, followed by change in voice3. On examination inspiratory stridor was most common finding. Out of total 6 tracheal narrowing cases most common presenting symptom was difficulty in breathing6, followed by change in voice4,and difficulty in swallowing2. On examination inspiratory stridor followed by biphasic stridor was significant. Graph 2: Distribution of cases based on symptomatology and site of narrowing
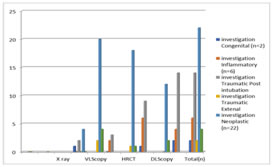
Out of 50 cases, both the congenital etiologies were identified by DL scopy and HRCT. Inflammatory conditions were best identified with HRCT. Video laryngoscopy was the best investigation to diagnose neoplastic and neurological conditions. For traumatic pathologies, both DL scopy and HRCT were equally efficient. VLscopy was helpful in external trauma cases. X ray had little significance. Graph 4: Distribution based on outcome of investigations
DISCUSSIONLaryngo-tracheal narrowing is an umbrella term, encompassing luminal compromise of the larynx (supraglottis, glottis, subglottis) and trachea. Pookamala S et al6 also reported post intubation laryngo-tracheal stenosis was the commonest cause comprising 38% of cases in their study. In an another study by Somu et al7 etiology of laryngo-tracheal stenosis in their case series was predominantly secondary to endotracheal intubation in 38 patients (71.69%), 11 patients (20.75%) were post-tracheostomy sequel, one patient had tracheal infiltration due to thyroid malignancy and had developed stenosis. This major difference in findings can be attributed to the lack of literature on present topic of research. In many studies conducted on laryngo-tracheal stenosis, authors have excluded the cases of malignancies. Myssiorek D. reported that vocal cord paralysis is most commonly iatrogenic or related to tumor infiltration, which is the main cause of change in voice, also observed as second common cause in present study. A clear etiology is not always found and recurrent laryngeal nerve injury may occur secondary to a number of pathologic processes, including vascular events, infections, drug toxicity, metabolic disturbances, or radiation therapy8.Common neoplasms identified as source of vocal cord palsy on imaging include thyroid neoplasms, submucosal mass with a predilection for the supraglottic and glottic regions, as seen in present study. Grenier P.A.et al. looked for etiology of stenosis in non-neoplastic cases and reported that TB, other infectious organisms like Klebsiella rhinoscleromatis, fungi, and particularly Aspergillus, may cause a tracheobronchitis in immunocompromised hosts, such as those with AIDS, underlying malignancy or post-transplant. They also reported inflammatory causes as Relapsing polychondritis, Wegener’s granulomatosis, and Broncholithiasis9. Other rare causes of airway stenosis were inflammatory bowel disease in which either ulcerative colitis or Crohn’s disease may produce airway inflammation. Most common etiology for laryngo-tracheal narrowing observed in present study was neoplasm (44%), followed by post-intubation trauma (28%). Other etiologies were inflammatory (12%), neurological (8%), congenital (4%) and external trauma (4%) Neoplastic pathologies were seen in 22 cases in present study, of which only 1 case of thyroid lymphoma was below 18 years. Slight male predominance was seen with 13 males (59.1%) to 9 females (40.1%). Most common clinical presentation of cases was difficulty in breathing 22 (100%) and change in voice 19 (86.4%). Biphasic stridor was noticed in 4 cases while 1 each had inspiratory and expiratory stridor. Most common site of narrowing was supraglottis (11/ 22 cases) followed by glottis (7/ 22 cases). In the present study, there were 12(54%) cases of primary laryngeal malignancy. Cases of non-laryngeal malignancy were 10(45%). Among non-laryngeal malignancy, there were 2 cases of thyroid, 3 mediastinal cases, 3 post cricoid cases and remaining 2 of hypopharynx, causing external pressure thereby leading to laryngo-tracheal narrowing. There was 1 (2%)case of benign neoplasia(recurrent respiratory papillomatosis) out of 23 cases under neoplastic etiology leading to laryngo-tracheal narrowing. Similar findings were observed by Ragheb AS.et al. in their study, they found that the distribution of laryngeal lesions of the included 40 patients;18 were laryngeal carcinomas (45%)8. In the present study, we tried to evaluate the association between the clinicoinvestigatory profile of the patients with the etiology involved in stenosis. The site and size of narrowing in both the congenital etiologies were best identified by both DL scopy and HRCT, but the measurement of distance of narrowing from laryngeal inlet was more accurately identified by DLscopy using zero degree endoscope and making specific markings on it from upper to lower limit of the lesion. Inflammatory conditions were best identified with HRCT. Video laryngoscopy was the best investigation to diagnose neoplastic and neurological and external trauma conditions. Though for post intubation traumatic pathologies, both DL scopy and HRCT were equally efficient, DLscopy gave more accurate results comparatively. Several diagnostic approaches have been used in patients with laryngo-tracheal stenosis, with some variability in practice patterns among major referral centres. Berrocal T.et al. also suggested that for congenital laryngo-tracheal stenosis, the criterion standard diagnostic modality is still direct laryngoscopy with rigid bronchoscopy10. Hofferberth SC. et al. in their study, “Management of Congenital Tracheal Stenosis” also suggested that the gold standard for definitive diagnosis of CTS is rigid laryngobronchoscopy under general anaesthesia. Direct visualisation of the airway enables accurate assessment of the length and diameter of the stenosed tracheal segment11. Ragheb AS et al. reported findings in accordance with the present study, neoplastic etiology was seen to best diagnose with virtual laryngoscopy. They reported that VL is an additive tool in conjunction with the direct laryngoscopy and easily reaches the lower limit of the lesion compared to direct laryngoscopy. CTVL could detect the laryngeal lesions with high sensitivity, specificity, and accuracy (95%, 100% and 96%, respectively)8.
CONCLUSIONThe most common etiology for laryngo-tracheal narrowing is neoplasm followed by post intubation trauma.Most common clinical presentation with laryngo-tracheal narrowing is difficulty in breathing, followed by change in voice, and difficulty in swallowing. For laryngo-tracheal narrowing cases with tracheal and congenital etiology like subglottic stenosis, direct laryngoscopy with 0 degree endoscope, is the best modality of investigation.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.