 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 3 - September 2019
Silenced by the Rooster - A case report
Rajarajeswari N1*, Paresh Naik2, Mary Kurien3, Arulmozhi4, Jayapriya5, Sajiev Koshy6, Sivaramakrishnan7
1Assistant Professor, 2Senior Resident, 3Professor and Head, 4,5Resident, Department of ENT, Pondicherry Institute of Medical Sciences, Pondicherry, INDIA. 2Professorand HOD, 7Assistant Professor, Department of Anaesthesiology, Pondicherry Institute of Medical Sciences, Pondicherry, INDIA. Email: rajisampathporal@gmail.com
Abstract Foreign bodies in the airway are common in otolaryngology practice especially in the paediatric age group. In adults, when encountered, are usually due to improper hasty ingestion, especially when intoxicated and cough reflexes are deranged. Foreign body in the airway is an emergency due to the risk of anoxia and death. Here, we are presenting a rare case of chicken bone stuck in the glottis and patient presented with inability to speak without breathing difficulty or dysphagia. We have discussed how we have approached this case without compromising patient safety. Key Word: Foreign body, Glottis, Aphonia.
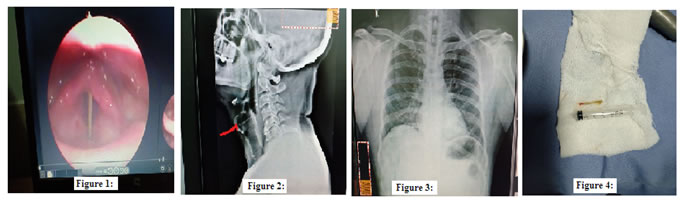
INTRODUCTION Foreign body in the glottis presents as a dire emergency and is mostly fatal before the person can reach medical care. Securing the airway during removal is a major concern. Laryngeal foreign body (FB) aspiration is more common in the paediatric age group.1 It’s presentation depends on the size, shape, site, nature of the FB and the degree of obstruction leading to a great variability of symptoms. The usual presentations are breathing difficulty, severe coughing, cyanosis and stridor. Complication rates of laryngeal FB increases with the duration of the FB in situ.2 General anaesthesia is usually preferred for FB removal using a rigid Laryngoscope. Here, we discuss about the unusual presentation of laryngeal FB and protocol followed for removal under local anaesthesia with the necessary pre and peri- operative precautions. CASE REPORT 43-year-old gentleman presented in the emergency with complaints of inability to speak following ingestion of chicken bone. At the time of ingestion, he had an episode of cough with minimal breathing difficulty for few seconds, following which he was comfortable with minimal pain in front of his neck and not able to speak. However, he was able to swallow well. There was no noisy breathing. Clinical examination revealed a comfortable patient, with aphonia but no stridor or drooling of saliva. Due to this unusual presentation, the patient was taken up for video laryngoscopy, promptly with a pulse oxy-meter. Around 1.5 cm long chicken bone was seen in the sagittal plane wedged in the glottis with adequate air gap between the bone and the vocal cords (figure 1). X ray soft tissue neck, lateral view revealed a linear radiopaque foreign body situated in the sagittal plane at the level of the larynx (figure 2). Chest X ray P-A view along with neck did not show any further abnormality (figure 3). The patient was immediately shifted to the operating room after taking consent for direct laryngoscopy and foreign body removal, along with the consent for tracheostomy and bronchoscopy in the event of any compromise of the airway, injury to glottis while instrumentation or bleeding, or slipping of the foreign into lower airway. Arrangements for the above additional procedures were also set up. Due to the critical position of the bone piece in the rimaglottidis, endotracheal intubation was deferred by the anaesthetist. In addition, the risk of aspiration was high, as patient had a full meal just half an hour prior. So, it was decided to take up the case under local anaesthesia with the anaesthetic team as stand by. Patient was given nebulisation with 4% Lignocaine and Budesonide for 10 minutes prior to shifting him on to the operating table. A nasopharyngeal airway was introduced for oxygenation with its tip at the level of nasopharynx. 10% lignocaine spray was used to the oropharynx, hypopharynx and larynx. Initial assessment was done using C-MAC video laryngoscope. 1.5cm long chicken bone was found wedged between the anterior and posterior commissures of the true vocal cords. Jackson’s rigid laryngoscope was introduced, and foreign body grasping crocodile forceps was used to remove the bone under vision, in toto (figure 4). Repeat laryngoscopy was done to check for any remnant FB, injury to the glottis or bleeding. Post removal, nebulisation was done with Budesonide, along with IV antibiotics and Dexamethasone. Patient was kept in the Intensive care Unit for observation and monitoring. Figure 1: Bone wedged in the glottic chink; Figure 2: Linear radiopaque foreign body in the saggital plane at the larynx; Figure 3: Normal Chest X-Ray; Figure 4: 1.5 cm long chicken bone removed. DISCUSSION Adult foreign body (FB) impactions in larynx are accidental in nature. Only two cases of glottic foreign bodies have been published. Kumkum et al. removed FB using anaesthetic laryngoscope with Magills forceps.3 Mundra et al in 2014 removed FB with ventilating bronchoscope without optical instruments.4 Airway foreign bodies are more common in the paediatric population. Usually they present with choking and stridor. However, the presentation can vary depending the size of the foreign body and the site of impaction. Kumar et al described in 2003, a case of an 8-month-old infant who presented with abnormal cry. A metallic blouse hook was noted sandwiching the vocal cords.5 As our patient had a unique presentation of loss of voice without respiratory distress, video laryngoscopy was done immediately, followed by X-rays of neck (PA and lateral view) and of chest to rule out another FB in lower airway besides assessing the airway. Laryngeal FBs have a risk of airway compromise due to faster onset of oedema and risk of dislodgement while manipulation, increasing chances of complications. Abhik Sikdar has described in 2017, a novel way of approaching an 11-month infant with history of aspirated broken metal toy. The FB was found to be a metallic foil at the level of the glottis extending to the subglottis. He preferred general anaesthesia with pre-tracheostomy where in trachea was exposed and stay sutures passed through anterior tracheal wall for immediate tracheostomy, if required6. CI NorHisyam et al. from University sains Malaysia Health Campus, reported a case of fish bone embedded in the right vocal cord which was removed under local anaesthesia, in 20177. In our paper, the peri-procedural concerns and preparations for an impacted foreign body larynx are being highlighted. Immediate rigid laryngoscopy and removal was necessary to reduce laryngeal oedema and onset of airway compromise. As patient was on full stomach and inadequate space for endotracheal intubation with possible dislodging of the foreign body further into the trachea, local anaesthesia was considered. 4% lignocaine with Budesonide nebulisation prior to the surgery with 10% lignocaine spray to the oropharynx, hypopharynx and larynx was used as it anaesthetises these areas for reduction of local pain and oedema. A pain-free, co-operative patient with reduced risk of airway compromise and bleeding was favourable. In an unfortunate event of airway compromise, bleeding or slippage of foreign body into the lower airway, alternative measures such as tracheostomy and bronchoscopy was mandatory and hence arranged. Gaining the confidence of the patient was an added crucial step in preparation under local anaesthesia and patient communication regarding details of the specific and alternative procedures was also done.
CONCLUSION A large foreign body in the glottic chink causing aphonia, without stridor is a rare occurrence. Immediate removal of the laryngeal foreign body, is mandatory to reduce onset of laryngeal oedema, airway compromise and catastrophic consequences. With confounding factors of patient on full stomach and possible dislodging the foreign body further into the trachea by endotracheal intubation, local anaesthesia is a safe alternative anaesthesia for laryngoscopy and removal of foreign body. Additional procedures of tracheostomy and/or bronchoscopy is indicated and need to be set up simultaneously considering any emergency airway compromise or in an unfortunate event of foreign body slipping into lower airway. Patient information regarding details of the specific / additional procedures including complications cannot be underestimated. A multidisciplinary approach with Anaesthetics on standby is mandatory for effective and safe patient outcome.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.