 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 2 - November 2019
Prevalence of haller cells - A retrospective observational study at a tertiary health care centre
Balaji Dhanasekaran1, Priya Kanagamuthu2*, Rajasekaran Srinivasan3, Paventhan K4, Prabakaran Somu4, Namasivaya Navin5, Ramya Shree C6
1,6Junior Resident, 2Professor, 3Professor and HOD, 4Assistant Professor, 5Senior Resident, Department of Otorhinolaryngology, Chettinad Hospital and Research Institute, Kelambakkam, Tamil Nadu, INDIA. Email: catchpriya.29@gmail.com
Abstract Background: Haller cells and it’s association with maxillary sinusitis have been a controversial topic. There is no definitive conclusion regarding the prevalence of maxillary sinusitis in the presence of Haller cells so far in the literature. Hence this study was conducted in our centre. Methods: A retrospective observational study conducted between March 2019 to July 2019 at the Department of ENT of 100 patients involving 200 maxillary sinuses at Chettinad Hospital and Research Institute, Kelambakkam Results: In our study the haller cells were found to be more prevalent in the age group between 31years to 40 years of age and was more prevalent in females. 17 of the patients had presence of Bilateral Haller cells in our study. 35.3% of the patients had associated maxillary sinusitis. The remaining 64.7% of the study patients did not have any radiological evidence of maxillary sinusitis. Prevalence of left sided haller cells were observed in 9 of the sample patients and about 55.6% of the same presented no signs of sinusitis in the maxillary sinus. Right sided haller cells were found in 16 patients and only 18.8% showed associated maxillary sinusitic changes. 58 patients had no radiological evidence of Haller cells in their respective CT PNS Conclusions: The presence of Haller cells alone is not a sole factor for the prevalence of maxillary sinusitis in our study. Thus, Haller cells may not be considered as an individual causative factor for maxillary sinusitis. Key Words: Haller cells, infraorbital ethmoidal air cells, paranasal sinuses, anatomical variations of paranasal sinuses
INTRODUCTION Haller cells are the anatomical variation in paranasal sinuses1 which were named after anatomist Albert Von Haller. He first identified this ethmoidal pneumatization of orbital floor in 1765. 1,2 The correct academic term according to the “International Conference on Sinus Disease” is “infraorbital ethmoid cell (Haller’s cell)” or “cellulae ethmoidales infraorbitales”,3 Haller cells are considered as an anterior extension of ethmoidal sinuses in to the orbital floor or superior aspect of maxillary sinus. They are located medial to the infraorbital canal and lateral to the nasolacrimal duct (Fig1). Haller cells themselves do not represent diseased state, but they can be responsible for patient symptoms.4 Infraorbital ethmoid cells have been described as well-defined, round, oval or teardrop-shaped radiolucencies (single or multiple), unilocular or multilocular with a smooth border which may or may not appear corticated, and are located medial to the infraorbital foramen.5 Large sized Haller cells can cause compression of infundibulum of maxillary sinus which may block muco ciliary flow, which will lead to disruption of transport and stagnation of fluid, which will produce favorable environment for bacterial growth which can further contribute to maxillary sinus diseases.5 The walls of the haller cells are thin and are often seen on CT scans through varying window settings. Haller cells are the anatomical variation in paranasal sinuses which can be seen in association with the other anatomical variations in osteo meatal complex such as concha bullosa, deviated nasal septum, and maxillary sinus septa. Haller cells are the anatomical variation in paranasal sinuses and not the pathology itself, but they can predispose some patient to sinus diseases by causing obstruction of the opening of the maxillary sinus that can lead to inflammatory disease. Therefore, the diagnosis of Haller cells by rhinologist becomes important to rule out the cause of sinusitis when no other significant finding on physical examination and endoscopy is seen in association with the disease. Detection of Haller’s cells may also forewarn the surgeons prior to endonasal procedures, thus preventing any untoward intraoperative complications.6 Diagnosis of Haller cells is mostly made with the aid of CT scans. They cannot be identified by Diagnostic Nasal endoscopy because of their location lateral to the infundibulum. A Haller cells is an anomaly that can narrow osteo meatal complex when larger in size which further will cause blockage of the sinus drainage pathway, which may result in inadequate sinus ventilation, vacuum headache, and pressure headache. These headaches are mostly located at frontal area followed by face and periorbital area. Only diseased haller cells or large haller cells block the ethmoidal infundibulum. Treatment is endoscopic resection of such cells.
MATERIALS AND METHODS Study Area: Department of Otorhinolaryngology, Chettinad Hospital and Research Institute. Sample size - 100 patients involving 200 maxillary sinuses. Study design – Retrospective observational study Inclusion Criteria:
Exclusion Criteria: 1. Patients with history of trauma. 2. Radiographic evidence of developmental anomalies / pathologies The institutional ethical clearance was obtained prior to the conduct of the study. Computed tomographic scans of the paranasal sinuses of 100 patients were observed retrospectively from March 2019 to July 2019. In our institute, the CT scan of paranasal sinuses were done using a Philips 128 Slice CT scan machine with slice thickness of 1.0mm. Axial and Coronal cuts were obtained. The presence of Haller cells was then identified. Haller cells were recognized by the criteria given by Mathew et al. (2013), as air‑filled cavities located medially on orbital floor and/or lamina papyracea, inferior to bulla ethmoidalis (large ethmoidal cell). Haller cells are surrounded by the ethmoidal capsule which distinguishes them from infra‑orbital recess of maxillary sinus. Haller cells can be of different sizes and shape, can be present unilaterally or bilaterally, and can be single in number or multiple. RESULTS TABLE1: Age group * Hallers cell prevalence Crosstabulation
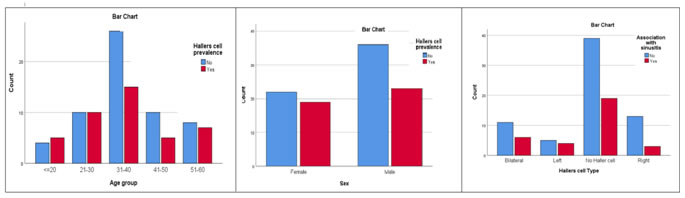
In our study the haller cells were found to be more prevalent in the age group between 31years to 40 years of age. It was noted that 36.6% of the individuals in the above mentioned age group had the infraorbital ethmoidal air cell. Table 2: Sex * Hallers cell prevalence Crosstabulation
About 39% males of thetotal patients in the study had Haller cells noted in their CT PNS. Females had a prevalence of 46.3% haller cells in the study.
Table 3: Hallers cell Type * Association with sinusitis
17 of the patients had presence of Bilateral Haller cells in our study. 35.3% of the patients had associated maxillary sinusitis. The remaining 64.7% of the study patients did not have any radiological evidence of maxillary sinusitis. Prevalence of left sided haller cells were observed in 9 of the sample patients and about 55.6% of the same presented no signs of sinusitis in the maxillary sinus. Right sided haller cells were found in 16 patients and only 18.8% showed associated maxillary sinusitic changes. 58 patients had no radiological evidence of Haller cells in their respective CT PNS Chi-Square Tests
a1 cells (12.5%) have expected count less than 5. The minimum expected count is 2.88.
DISCUSSION Bolger et al. Reported equal prevalence of Haller’s cells in cases with and without sinus disease was noted in the studies.10 Milczuk et al. 11 reported Haller’s cells associated with ipsilateral sinus disease in 66.7% of their patients. Earwaker12 reported that sinus diseases can occur equally in patients with Haller cells and without Haller cells. Wanamaker[14] reported the case of headache and sinus disease because of Haller’s cell. Sebrechts et al. [13] found Haller cells as one of the etiologic factor in maxillary sinusitis certainly when the cells are large enough to cause ample narrowing of maxillary infundibulum. Mathew et al. 15 using CBCT demonstrated in their study that there is no significant association between Haller cells and ipsilateral maxillary sinusitis. In our study, the haller cells were found to be more prevalent in the age group between 31years to 40 years of age and was more prevalent in females. 17 of the patients had presence of Bilateral Haller cells in our study. 35.3% of the patients had associated maxillary sinusitis. The remaining 64.7% of the study patients did not have any radiological evidence of maxillary sinusitis. Prevalence of left sided haller cells were observed in 9 of the sample patients and about 55.6% of the same presented no signs of sinusitis in the maxillary sinus. Right sided haller cells were found in 16 patients and only 18.8% showed associated maxillary sinusitic changes. 58 patients had no radiological evidence of Haller cells in their respective CT PNS.
CONCLUSION The presence of Haller cells alone is not a sole factor for the prevalence of maxillary sinusitis in our study. Thus, Haller cells may not be considered as an individual causative factor for maxillary sinusitis.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.