 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 3 - December 2019
Study on bipolar cautery assisted dissection of superior pole in tonsillectomy surgeries
P K Purushothaman1, C R K Balaji2*, Manoj Pandian3, Premnath4
1Professor and HOD, 2Associate Professor, 3Post Graduate, 4Senior Resident, Department of ENT, SRM Medical College Hospital and Research Centre, SRM nagar, Potheri, Kattankulathur, Kancheepuram district, Tamil Nadu, INDIA.
Abstract Aims and Objectives: The aim of the study is to describe the effectiveness of using bipolar cautery in identifying and dissecting the tonsillar capsule of superior pole instead of waugh forceps in cases of tonsillectomies in our institution. Study design: Retrospective study. Study period: June 2013 to June 2018. Setting: SRM Medical College Hospital, Kattankulathur. Patients: A total of 450 patients were included who underwent tonsillectomy. Patients were grouped into two, one group with using Waugh’s toothed forceps and another group using bipolar cautery for incision and identifying the tonsillar capsule and dissecting the tonsillar capsule of superior pole of tonsils during tonsillectomy. Results: The easy identification of tonsillar capsule and dissection of capsule of superior pole without much bleeding and reduction in the overall surgical time was observed in patients, when bipolar cautery was used in tonsillectomy surgery.(no. of patients in both groups) Conclusion: There are various methods of tonsillectomy procedures. There are lots of techniques as well in the conventional methods. As the famous Aristotle saying “Well begun is half done” the identification of the tonsillar capsule and proper dissection of superior pole ensures the proper dissection plane and this method of using bipolar cautery helps us in early identification of the tonsillar capsule and proper dissection of the superior pole from the appropriate plane. Key Word: bipolar cautery.
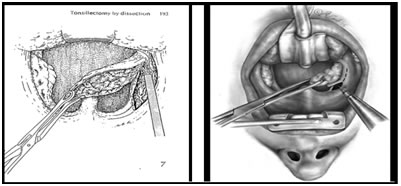
INTRODUCTION The right and left palatine tonsils form part of the circumpharyngealwaldeyer lymphoid ring. Each tonsil is an ovoid mass of lymphoid tissue situated in the lateral wall of the oropharynx. They usually reach a maximum at puberty, when they average 20–25 mm in vertical, and 10–15 mm in transverse, diameters, and they project conspicuously into the oropharynx. Tonsillar involution begins at puberty, when the reactive lymphoid tissue begins to atrophy, and by old age only a little tonsillar lymphoid tissue remains. Its medial, free, surface usually presents a pitted appearance. The pits, 10–20 in number, lead into a system of blindending, often highly branching, crypts that extend through the whole thickness of the tonsil and almost reach the connective tissue hemicapsule. In a healthy tonsil, the openings of the crypts are fissure like and the walls of the crypt lumina are collapsed so that they are in contact with each other. The lateral or deep surface of the tonsil spreads downwards, upwards and forwards. Inferiorly, it invades the dorsum of the tongue; superiorly, it invades the soft palate; and, anteriorly, it may extend for some distance under the palatoglossal arch. This deep, lateral aspect is covered by a layer of fibrous tissue, the tonsillar hemicapsule. The latter is separable with ease for most of its extent from the underlying muscular wall of the pharynx, which is formed here by the superior constrictor. Anteroinferiorly, the hemicapsule adheres to the side of the tongue and to palatoglossus and palatopharyngeus. In this region, the tonsillar artery, a branch of the facial artery, pierces the superior constrictor to enter the tonsil, accompanied by venae comitantes. Each tonsil is a mass of lymphoid tissue associated with the oropharyngeal mucosa and fixed in its position, unlike most other examples of mucosa associated lymphoid tissue. It is covered on its oropharyngeal aspect by nonkeratinized stratified squamous epithelium. The whole of the tonsil is supported internally by a delicate meshwork of fine collagen type III (reticulin) fibres which are condensed in places to form more robust connective tissue septa that also contain elastin. The epithelium lining the crypts is mostly similar to that of the oropharyngeal surface, i.e. stratified squamous, but there are also patches of reticulated epithelium, which is much thinner, and which has a complex structure that is of great importance in the immunological function of the tonsil. The lymphoid tissue of the reticulated crypt epithelium contains pre dominantly IgG and IgA producing B lymphocytes, T lymphocytes and antigen presenting cells. The arterial blood supply to the palatine tonsil is derived from branches of the external carotid artery which include Tonsillar branch of facial artery which is the main artery, Ascending pharyngeal artery from external carotid, Ascending palatine, a branch of facial artery, Dorsal linguae branches of lingual artery, Descending palatine branch of maxillary artery. The tonsillar region is innervated by tonsillar branches of the maxillary and glossopharyngeal nerves. The organism most commonly identified from the surface of the tonsil in disease is the group A beta haemolytic streptococcus (GABHS).Acute inflammatory episodes affecting the tonsils may occur as an isolated episode, or in association with a viral upper respiratory illness including generalized pharyngitis (see Figures 95.1 and 95.2). Tonsillitis may also present as part of a systemic infection such as infectious mononucleosis. The diagnosis of acute tonsillitis is clinical. It is based on a history of a pyrexial illness, sore throat with a painful swallow, and the finding of pharyngeal erythema with or without tonsillar exudates and painful cervical adenopathy. patients complain of chronic low- grade symptoms affecting their quality of life because of throat discomfort, and the production of unpleasant smelly white or yellow debris from the tonsillar crypts. Rarely, this debris may become inspissated, calcify and form a tonsillolith, which may itself be complicated by acute sepsis. The commonest indications for tonsillectomy is recurrent infections of throat which can be seven or more episodes in 1 year, or Five episodes per year for 2 years, or Three episodes per year for 3 years, Peritonsillar abscess, tonsillitis resulting in febrile seizures. Tonsillectomy must also be performed after one quinsy, preferably 4-6 weeks after the acute infection has subsided; and it should be considered in patients who have recurrent attacks of acute rheumatism or nephritis and in those who are stubborn carriers of streptococci or diphtheria bacilli. Tonsillectomy is sometimes necessary in adults when enlargement of one tonsil without ulceration demands the exclusion of malignancy. Tonsillectomy should never be undertaken without very good reason in those with a known bleeding diathesis, such ashaemophilia. The patient is placed supine, with the head slightly extended. The Boyle-Davis gag is introduced and opened, with the tongue blade in the midline. The gag is secured in the optimum position with Draffin's bipods. The tonsil is grasped with Denis brown forceps and drawn firmly in a medial direction, thus exposing an area of mucosa medial to the free edge of the anterior faucial pillar. The incision is started halfway between the upper and lower 'poles' of the tonsil, instrument waugh forceps being inserted to the depth of the surgical 'capsule' of the tonsil, the surgeon carries the incision downwards to the base of the tongue and upwards to the upper pole. When the capsule has been identified, a MollisonPillar retractor is used to separate the tonsil and its capsule from the surrounding peritonsillar tissues. The upper pole must first be mobilized, care being taken to keep the dissector as close as possible to the capsule throughout the dissection. Gripping the tonsil by its upper pole, the surgeon continues to draw the tonsil towards the midline, and extends the dissection by separating the peritonsillar tissues from the capsule, until the lower pole is approached. Towards the lower pole of the tonsil there is a firm fibrous triangular fold which tends to hold up the dissection at this point. The triangular fold should be cut with scissors and the dissection carried on to the base of the tongue. A Tonsillar snare is threaded over the tonsil, which is finally removed by closing the snare at the level of the tonsillolingual sulcus. This ensures that the tonsils removed in total, Failure to do so may result in 'recurrence.
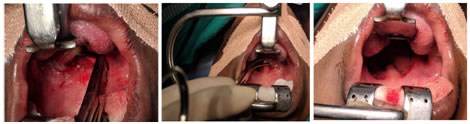
MATERIALS and METHODS This retrospective study was conducted in SRM Medical college hospital and research institute, Chennai, from June 2013 to June 2018. A total of 450 patients with chronic tonsillitis, who were admitted in the department of Otorhinolaryngology were analyzed during the study period. Cases with indications for tonsillectomy were selected. All cases who had contraindications for the surgery were excluded. All cases underwent a thorough history taking and detailed clinical examination. Basic blood and urine test were done. One group had tonsillectomy with capsular identification and dissection of superior pole using waugh forceps and the other group with capsular identification and dissection using bipolar cautery with an electrocautery setting of 20w. The assessments were made on duration of surgery, early and easy identification of plane of dissection and the number of cotton balls used and the results analyzed.
RESULT There were 225 people with superior pole dissection done using waugh forceps dissection of superior pole and 225 people with superior pole dissection done bipolar cautery dissection of superior pole. The Average duration of surgery for using bipolar was35 minutes while that using waugh forceps was 45 minutes and number of cotton ball usage in cases done with bipolar cautery was 15-20 while in cases done with waugh forceps dissection was 30
DISCUSSION Among 450 patients who had surgery, 225 underwent dissection of superior pole using bipolar cautery; 225 underwent dissection of superior pole using waugh forceps. We assessed the average duration of surgery and the number of cotton balls for patients who underwent surgery with bipolar cautery technique for capsular identification and dissection of superior pole and patients who underwent surgery with waugh forceps for capsular identification and dissection of superior pole. We also assessed the number of cotton balls used in cases done with dissection of superior pole using bipolar cautery and waugh forceps. There are studies which assessed Using an electrocautery setting of approximately 20 W (if using a standard electrocautery tip) or 6 W (if using a microdissection needle), the anterior tonsillar pillar is incised, and the entire palatine tonsil with the capsule is dissected from surrounding tissue (5). This study found that the duration of surgery and number of cotton ball used were less in cases done with dissection of superior pole using bipolar cautery than those done with waugh forceps. CONCLUSION There are various methods of tonsillectomy procedures. There are lots of techniques as well in the conventional methods. As the famous Aristotle saying “Well begun is half done” the identification of the superior pole ensures the proper dissection plane by using bipolar cautery helps us in identifying the tonsillar capsule of the superior pole easily.
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.