 Home
Home
|
Table of Content - Volume 13 Issue 1 - January 2020
A case report on external auditory canal osteoma
B C Patil1, Deepal Kundu2*, R S Mane3, A A Mohite4, V V Varute5, Ganesh Tarlekar6
1 Professor and Medical Superintendent, 2Junior Resident, 3HOD and Professor,4Associate Professor, 5Assistant Professor, 6Senior Resident, D.Y.Patil Hospital and Research Institute, Kolhapur, Maharashtra, INDIA. Email: drbalasahebpatil6@gmail.com, kundudeepal92@gmail.com, manerajashri45@gmail.com, dranjanamohite@gmail.com
Abstract External auditory canal osteomas are benign osseous tumors. They are unilateral, solitary, slowly growing. Clinical presentation ranges from mostly being asymptomatic to hearing loss, otalgia, tinnitus, ear fullness. External auditory canal osteomas must be differentiated from External auditory canal exostosis. Radiological and Histological investigations will confirm diagnosis. Surgical excision is definitive treatment. Osteomas have excellent prognosis. We present a case report of 22 year old female with External auditory canal osteoma in left ear. Key Words: External Auditory Canal, Exostosis, Osteoma, Radiological, Histopathological
INTRODUCTION External auditory canal obstruction is a very common condition presenting to otorhinolaryngologists. External auditory canal osteoma is a very rare cause of it. External auditory canal osteomas are found to be very rare bony benign neoplasms which are usually asymptomatic, unilateral, solitary, slowly growing.1 They have predilection for External auditory canal, Mastoid cortex, Facial bones, Mandible 2. External auditory canal osteomas and Exostosis share a similar clinical picture. We present a case of Left external auditory canal osteoma.
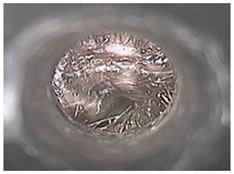
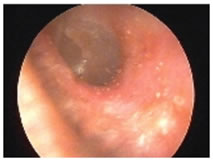
CLINICAL CASE A 22 year old female presented with chief complaints of left ear pain since 15 days and left ear diminished hearing since 15 days. There was no history of vertigo/tinnitus/trauma/water sports. On ear examination, left external auditory canal was partially obstructed by a hard mass which was fixed and covered with wax. Surrounding skin of External auditory canal was normal. Left tympanic membrane was partially visible. Right ear was normal. Pure tone audiometry revealed conductive hearing loss in left ear. Hearing was normal in right ear. HRCT Temporal Bone revealed oval shaped well defined bone density lesion of size 7x4mm along inferior wall of left external auditory canal. Provisional diagnosis of Left external auditory canal osteoma was made. Osteoma was surgically excised through its pedicle and was sent for histopathology which revealed bony lamellae surrounded by fibrovascular channels. This confirmed diagnosis of left external auditory canal osteoma.
DISCUSSION Osteomas are benign tumors which are made up of mature bone and are slowly growing. In Head and Neck region, Fronto-ethmoidal region is the most common site of their occurrence. In temporal bone, osteoma is very rare with highest predisposition for external auditory canal (usually from tympanomastoid and tympanosquamous suture line)3. Incidence is estimated to be 0.05% of all ear surgeries 4. External auditory canal osteomas are non invasive, however, External auditory canal obstruction can cause significant symptoms like hearing loss, ear fullness, tinnitus, ear pain 5. Osteomas of External auditory canal are very rarely complicated by External auditory canal cholesteatoma with only few reports in current literature 6. Although, exact mechanism for formation of osteoma is unknown, various etiologies have been proposed till now like persistent embryonic periosteum, congenital origin, trauma and muscle traction, hormonal 7. Gardner’s syndrome may present with multiple osteomas 9. External auditory canal osteomas must be differentiated from External auditory canal exostosis as both share similar clinical symptoms 5. Radiographically, osteoma is characterized by hyperdense mass which is single, unilateral, pedunculated arising from tympanomastoid and tympanosquamous suture line whereas exostosis appears as hyperdense mass protruding in internal auditory canal – multiple, bilateral, smooth bordered, broad based without deep extension 9. Histologically, External auditory canal osteomas are composed of lamellated bone with minimal osteocytes surrounded by fibrovascular channels. In contrast, Exostoses are characterized by parallel, concentric layers of subperiosteal bone with abundant osteocytes 9. Graham et al concluded that presence or absence of fibrovascular channels is distinguishing histological difference between External auditory canal osteoma and External auditory canal exostoses 10. According to a recent study conducted by Fenton et al, osteoma and exostoses can’t be diffentiated histologically as even exoxtoses can have fibrovascular channels 11. External auditory canal osteoma and External auditory canal exostoses should be surgically treated 5. External auditory canal osteomas have low recurrence rate and have no predilection for malignancy 12.
CONCLUSION External auditory canal osteomas are benign and asymptomatic. Canal obstruction will produce symptoms. Complete surgical excision through its stalk is definitive treatment to avoid recurrence 13. Prognosis is excellent 5.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.