 Home
Home
|
Table of Content - Volume 13 Issue 3 - March 2020
Surgical removal of a large branchial cyst of the second cleft: A case report
Francesco Asprea1*, Giuseppe Russo2, Gregorio Micali3, Giulia Lucchesi4, Carlotta Corpina5, Gianfranco Lenzo5, Maria Gabriella D’Arrigo5, Francesco Carfì6
1Head, 4Co- Director, 6Senior Consulting, Division of Otolaryngology C.O.T. Clinic – Via Ducezio, 1, Messina, Italy. 2Head Of Division, 5Co-Director, Division of Anesthesiology And Intensive Care, C.O.T. Clinic – Via Ducezio,1, Messina, ITALY. 3Co- Director of Division of Otolaryngology, Head Of The Maxillofacial Surgery Unit C.O.T. Clinic – Via Ducezio, 1, Messina, ITALY. Email: ciccioasprea@gmail.com
Abstract Background: In this work, the Authors present a case of voluminous branchial cyst classifiable as type II according to Bailey operated in June 2018 with excellent functional and aesthetic results and without a recurrence evident 18 months after surgical treatment. The Authors consider the correct preoperative classification and classification of these dysembriopathies to be essential for successful surgical treatment. Key Words: Cyst, Branchial, second cleft, surgery.
INTRODUCTION Hunczowski (19) in 1789 first described a branchial cyst, while it was Langenbeck in 1859 who first described its surgical treatment. Bailey 7, 8 in 1922 classified the cysts of the second branchial fissure into four stages. In 1972 Work (43) classified the branchial anomalies of the first fissure into two types. In this work a case of large cyst of the second branchial cleft of the second type according to Bailey is presented.
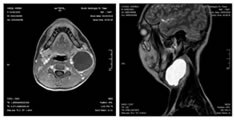
MATERIALS AND METHODS We present a case of a 17 year old young man who came to our observation for a voluminous left lateralocervical swelling. A CT and an MRI with contrast medium defined the anatomical limits of the swelling and its compression ratios towards the vascular-nervous axis of the neck ( fig. 1, 2).
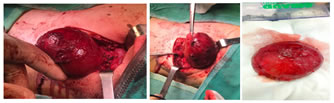
Figure 1, 2: RMN imaging The preoperative diagnosis was of branchial cyst classifiable as cyst of the second branchial fissure of type II according to Bailey 6,8. The dimensions of the mass were about 8 centimeters in diameter and the shape almost spherical. The surgery took place under general anesthesia with oro-tracheal intubation and lasted two hours and thirty minutes. The excision of the mass was complete without residues and without intraoperative bleeding ( fig. 3, 4, 5, 6, 7). The surgical wound was sutured with intradermal suture after affixing drainage and aspiration which was removed 48 hours after surgery. The day after the drain was removed, the patient was discharged. The postoperative course did not present complications. After more than 18 months from the surgery there were no recurrences and the functional and aesthetic result can be defined as excellent.
Figure 3,4,5,6,7: Surgical imaging
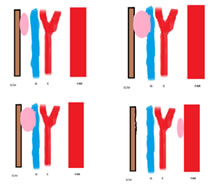
OBSERVATIONS AND RESULTS Starting from the end of the fourth week of gestation, six pairs of branchial arches are differentiated in the human embryo, consisting of mesenchymal tissue covered externally by ectoderm and internally by endoderm. Each arch corresponds internally with an endodermal branchial pocket and externally with an ectodermal branchial sulcus 1,2,3,4,5,6,9,10,11,12,13. The second branchial arch extends downward into the neck to cover the second, third and fourth branchial sulcus, forming His's cervical sinus; Reickert's cartilage differs from the center of the arch, which will form the upper part of the hyoid bone. Overall, the stirrup, the styloid process, the upper body and the small horn of the hyoid bone, the posterior belly of the digastric muscle, the mimic muscles, the stapedius muscle, the facial nerve and the stapedial artery will derive from the second arch. Palatine tonsils will form from lymphocytic colonization of the second branchial endodermal pocket. A correct knowledge of embryology of the branchial arches is essential for a correct diagnosis and correct treatment of the anomalies that derive from them, which are classified according to the arch, pocket or furrow from which they derive; the correct knowledge of these derivations and of the structures connected embryologically and anatomically to the anomalies allows a treatment of the same that provides a complete surgical resection avoiding iatrogenic damage to the surrounding structures 14, 15, 16, 17,18,20,21,22,23,25,26,27. Branchial anomalies, according to their embryological origin, can be lined internally with squamous or respiratory epithelium in the context of which lymphoid or sebaceous or salivary tissue can be found and contain a mucous fluid with cholesterinic crystals. Cysts, fistulas and sinuses can be distinguished. The cysts are reliquaries of the branchial structure without external opening. The sinuses are reliquaries of a branchial structure with external opening but without internal opening, while the fistulas are determined by the complete persistence of the branchial structure with interruption of its membranes so as to determine a pharyngocutaneous fistula; it is therefore necessary, in the clinical evaluation of these anomalies, to insert an endoscopic evaluation of the upper aero-digestive tract in order to identify the pharyngeal opening that can be localized at the level of the tonsil fossa or pyriform sinus24,28,29,30,31,38. Cytological diagnosis by needle aspiration 41 can be useful to confirm the diagnosis, especially in adults, where the possibility of a metastatic localization must also be taken into consideration, a rarer possibility in childhood; the diagnosis and the correct preoperative evaluation of the lesion extension will be facilitated by the ultrasound study, the CT and the MRI, while in the case of suspected anomaly of the third and fourth arch with opening in the pyriform sinus, the esophagogram with bary meal may be useful 32,33,34,35,36,37,39,40,42. The treatment of these lesions is surgical, also considering the possibility of neoplastic degeneration and the frequent infectious episodes, which make radical excision more difficult and facilitate recurrence. Abnormalities of the second branchial cleft are the most common and make up about 90% of the total branchial anomalies. Considering the anatomical structures that originate from the second branchial arch and from the second pocket, it is understood how these anomalies can contract relationships with the supratonsillar fossa where they can open via fistulosis and how they contract relationships of close contiguity with the glossopharyngeal nerve and the hypoglossal nerve nearby from the supratonsillar fossa itself. Bailey 7,8 in 1922 classified the anomalies of the second branchial cleft in four degrees according to their relationship with the vascular-nervous bundle of the neck. Type I includes lesions located anteriorly to the sternocleidomastoid muscle without contact with the carotid axis Type II includes lesions located deep with respect to the sternocleidomastoid muscle and anteriorly or posteriorly to the carotid axis; they are the ones most frequently found among the anomalies of the second crack Type III includes lesions that are located in the bifurcation between the external carotid and internal carotid adjacent to the pharynx Type IV includes lesions located deep with respect to the carotid axis, near the pharynx and adjacent to the supratonsillar fossa (Fig. 8, 9,10,11)
Figure 8,9,10,11: Tipes I, II, II,IV sec Bailey ( from Asprea F. Le tumefazioni del collo in età pediatrica, Phasar Ed. Italy, 2016)
The clinical presentation of the anomalies of the second fissure is that of a mass localized in the neck in front of the anterior margin of the sternocleidomastoid muscle that can increase in volume or even give a sign of itself for the first time, after a phlogistic fact of the first aero -digestive routes 6. These are clearly anomalies present at birth but a first diagnosis in adulthood is not rare, often in the third or fourth decade of life as the gill epithelial inclusions are likely to be originally small and clinically inapparent to then grow and give a sign of themselves after phlogistic facts. In these cases, problems of differential diagnosis arise, especially in adulthood, with metastases colliquated by carcinomas of the upper aero-digestive tract or with salivary or hydatid cysts of the parapharyngeal space, so before any surgical decision it is advisable to carry out a clinical examination of the entire upper aero-digestive tract, an evaluation by CT and MRI with contrast medium of the head-neck district and a possible cytological confirmation by aspiration if deemed necessary from the clinical point of wiew 14,18 Fistulas, on the other hand, are more frequently diagnosed in childhood and are clinically highlighted by a chronic drainage of purisimilar fluid from a fistula located in the lower third of the neck in front of the anterior edge of the sternocleidomastoid muscle. The treatment of these anomalies is surgical 6. The cysts of the second fissure are surgically approached through a transverse incision along a natural fold of the neck; a careful and delicate dissection is carried out along the walls of the cyst taking care not to break them, an event often facilitated by the subtlety of the walls themselves and which makes dissection more difficult; it is good to carry out a careful search for an eventual associated fistula which, if present, must be included in the excision to obtain a complete removal of the branchial anomaly preventing recurrence. The hypoglossal, vagus and spinal nerves must be identified and respected; at a certain point of the dissection, having reached the upper part of the cyst, it is necessary to take into account the relationship with the tonsil dimple and dissect up to the same and for this purpose the insertion of a gloved finger into the oropharynx by the anesthesiologist or an assistant it can be useful, by exerting a downward pressure starting from the tonsillar region, to identify the fistula which must be sectioned and tied to the entrance of the fossa; in some cases it may be necessary to associate a tonsillectomy. The difficulty of this intervention increases, passing from the I and II sec Bailey types to the III and IV types, in the latter two cases, a dissection of the cyst must be carried out from the jugulo-carotid vascular structures to which it can also appear very adherent with risk of vascular injury. In the case of fistulas, their outlet on the anterior edge of the sternocleidomastoid must be identified; the outlet must be circumscribed by means of a semilunar incision and from there it must be followed upwards with a careful dissection; a second horizontal incision at the level of the hyoid bone allows to follow the passage even higher, in its passage under the digastric muscle and up to the carotid bifurcation, where it is tied and sectioned.
CONCLUSIONS In the case of branchial anomalies, the correct pre-operative diagnostic framework and the correct classification based on embryological knowledge allows for surgical treatment which in expert hands is free from complications and relapses; a cautious and anatomically correct surgical approach allowed a brilliant and uncomplicated result.
REFERENCES
Policy for Articles with Open Access
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.