 Home
Home
|
Table of Content - Volume 14 Issue 1 - April 2020
A retrospective study of neonatal and perinatal factors affecting transient evoked otoacoustic emissions in newborn hearing screening in a tertiary care hospital
Ravikeerthi G1*, Norma Thomas2
1Assistant Professor,2Post Graduate Department of ENT, Sapthagiri Institute of Medical Science and Research Centre, No. 15, Chikkasandra, Hesarghatta main road, Bangalore – 560090 INDIA.
Abstract Background: TEOAE have been widely used in neonatal hearing screening. TEOAE has advantage of being stable, fast and non-invasive, enabling cochlear integrity monitoring. Objective: To study neonatal and perinatal factors affecting TEOAE in new born hearing screening. Material and Methods: A retrospective study was conducted in all new-borns came for new born hearing screening in ENT OPD, Sapthagiri institute of medical science, Bangalore from January 17 to January 19. After written informed consent was obtained, the subjects were brought to the test room, and an OAE test was administrated by audiologist. All the new-borns were undergone detailed work up including detailed maternal and perinatal history. The study was done after obtaining institutional ethical committee approval. Result: In our study we took neonatal factors like gestational age and birth weight, and maternal factors like maternal age, consanguinity and mode of delivery, and its relation to OAE. With respect to gestational age, Term babies showed better responses than preterm. With respect to maternal age, babies born to mothers more than 30 year old showed more REFER result than mothers who were under 30. Conclusion: TEOAE has advantage of being stable, fast and non-invasive, enabling cochlear integrity monitoring. This test can be performed easily in new-borns irrespective of gestational age. Keywords: TEOAE- TRANSIENT EVOKED OTOACOUSTIC EMISSIONS.
INTRODUCTION Hearing loss is not uncommon in children. The incidence of severe hearing impairment in neonates has been estimated to be about one in 700 to 1100. In 1990, the joint committee on new born hearing recommended that new born with specific high risk factors should receive audio logical screening to have habilitation begun by 6 months of age. Several studies suggest that Evoked otoacoustic emission (EOAE) testing is fast and reliable enough to be potentially cost effective method for screening all neonates for hearing disorders. In 1978, Kemp demonstrated the existence of Otoacoustic emissions(OAEs) by using a small microphone placed within the external ear canal to record an acoustic response 5 milliseconds following a click stimulus. In recent years, The recording of TEOAE has been widely used in neonatal hearing screening of new-borns without hearing risks, using low intensity stimuli, with a widelange of frequencies and in short period of time. In recent study the authors evaluated differences in the Otoacoustic emissions full term and preterm new-borns, and found higher response latency in preterm infants. OAEs are measured by presenting a series of sounds to the ear through a probe that is inserted in the ear canal. The probe contains a loudspeaker that generates the sounds and a microphone that measures the resulting OAEs that are produced in the cochlea and are transmitted through the middle ear into the outer ear canal. The resulting sound that is picked up by the microphone is digitized and processed by the instrument. Otoacoustic emissions (OAE) hearing screening, used widely in hospital-based new born hearing screening programs, represents a significant advance for screening young children. An objective method that screens hearing in a range of sound frequencies critical for normal speech and language development, portable OAE screening is the most practical method for screening infants and toddlers because it:
CLINICAL STRENGTHS AND WEAKNESSES Research on the application of OAEs in new born hearing screening has contributed to widespread appreciation of their multiple clinical advantages and, also, the recognition of some clinical disadvantages. Strengths for any clinical procedure are invariably tempered, to some extent, by clinical weaknesses. Some strengths and weaknesses of OAEs as a technique for new born hearing screening are summarised as follows: STRENGTHS
WEAKNESSES
MATERIALS AND METHODS A retrospective study was conducted in all new-borns came for new born hearing screening in ENT opd, sapthagiri institute of medical science, Bangalore from January 17 to January 19. After written informed consent was obtained, the subjects were brought to the test room, and an OAE test was administrated by audiologist. All the new-borns were undergone detailed work up including detailed maternal and perinatal history, thorough clinical examination of ear, nose and throat. The study was done after obtaining institutional ethical committee approval. PROCEDURE The new born was brought to the test area and placed in mother's lap in a sound proof room to minimize external sounds. The test room was a part of audiology room designated for screening. Adaptations made to limit low-frequency background noise included acoustic tiles and room dividers. Noise in the room was produced by quiet conversation, moving of neonates, and the operation of the keyboards. The computer-based analyser was used to record click-evoked OAEs from each ear with a standardized procedure. A small acoustic probe fitted with a rubber tip was introduced into the ear canal. An attempt was made to obtain the best possible probe fit while maintaining a quiet new born state. Probe fit was evaluated by measuring an adequate stimulus across the entire 0.5- to 5-kHz frequency range and setting the stimulus gain to obtain an average paediatric sound pressure level of 80 dB (or 40-dB spectrum level). Stimuli were 80-microsecond rectangular pulses generated by a 12-bit digital to analog converter and presented at 50 clicks per second through a miniature transducer housed in the probe. A miniature microphone also was housed within the probe. If the device detects OAEs, the result is displayed as "PASS". If no response is detected, the result is a "REFER" which does not necessarily mean that there is a hearing loss present. "REFER" means that further tests are needed to verify if a hearing loss is present. INCLUSION CRITERIA: EXCLUSION CRITERIA:
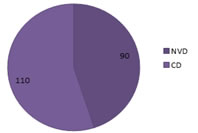
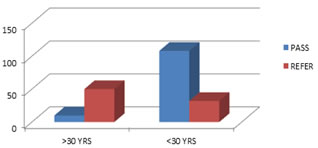
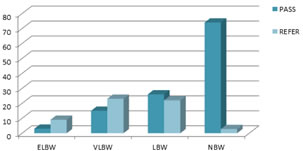
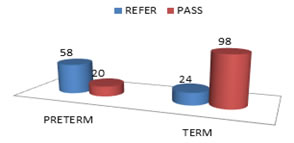
RESULTS: Out of 200 new-borns that were taken for study 108 were males and 92 were females. Out of 200, 22 neonates were born to consanguineous couple. In that 27.2% showed PASS result.72.6% showed REFER. 200 New-borns divided according to gestational age into preterm ( < 37weeks)and term (>37 weeks).out of 200, 78 were preterm and 122 were term.80.3%of term babies showed pass and 19.6%showed refer. 25.6% of preterm showed PASS. 74.3% of preterm showed REFER result. 200 new-borns grouped I the basis of birth weight.102 new-borns had normal birth weight (2.5 kg-3.5kg),In new-borns with normal birth weight ,72.5% showed PASS .27.4% showed REFER. Out of 12 new born with extremely low birth weight, 75% showed REFER. Only 25% showed PASS. In VLBW new-borns 60.5% showed REFER and 39.4% showed PASS. In LBW new-borns 54.1% showed PASS and 45.8% showed REFER. On the basis of maternal age factor, 200 new-borns grouped into 2 categories, one group with maternal age >30 years. other group with maternal age<30 years. Out of 200 newborns, 140 were born to mothers with age less than 30 years. In this 77.1% showed PASS .22.8% showed REFER. Only 60 out of 200 were born to mothers more than 30years. In this 83.3% showed REFER. Only 16.6% showed PASS result. Out of these 200 new-borns , 90 were born by normal vaginal delivery, in that 10 were preterm and 80 were term babies. Out of 110 babies delivered by C section ,68 were preterm and 42 were term. Preterm babies showed more REFER results compared to term babies. Figure 1: Graph depicting sex preponderance
Figure 2: Graph showing consanguinity
Figure 3: Graph depicting mode of delivery
Figure 4: Graph depicting maternal age and OAE results.
Figure 5: Graph depicting birth weight and OAE results
Figure 6: Gestational age and OAE results CONCLUSION TEOAE have been widely used in neonatal hearing screening .TEOAE has advantage of being stable, fast and non-invasive, enabling cochlear integrity monitoring. This test can be performed easily in new-borns irrespective of gestational age. From the result analysis we concluded that in comparing genders an ears, there was no difference in result between genders and right and left ears. In our study we took neonatal factors like gestational age and birth weight, and maternal factors like maternal age ,consanguinity and mode of delivery , and its relation to OAE. With respect to gestational age, there was significant change in result of OAE. Term babies showed better responses than preterm. With respect to maternal age, babies born to mothers more than 30 year old showed more REFER result than mothers who were under 30 . In our study 22 new-borns were born to consanguineous couple. In that 68.1% showed REFER .31.8% showed PASS result. With respect to birth weight and mode of delivery, new-borns with very low birth weight and low birth weight showed more REFER result compared to new-borns with normal birth weight. New born born by caesarean delivery showed higher failure rate on OAE compared to vaginally delivered newborns.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.