 Home
Home
|
Table of Content - Volume 14 Issue 3 - June 2020
A study on efficacy of budesonide nasal irrigation in post-operative fess
P K Purushothaman1, U Prem Aanand2, D Anand Karthikeyan3*, Siva Ranjani4
Department of Otorhinolaryngology, SRM Hospital & Research Institute, Kattankulathur, Kanchipuram 603203. Email: premdebull@gmail.com
Abstract Background: To compare the efficacy of budesonide and normal saline nasal irrigation in post-operative management of functional endoscopic sinus surgery Method: A prospective, randomised controlled study was done in the Dept. of Otorhinolaryngology, SRM medical college hospital and research centre, kaatankulathur Aim: To compare the efficacy of budesonide and normal saline nasal irrgation in post-operative management of functional endoscopic sinus surgery patients from 2017 to 2019. Results: Eighty (80) patients with chronic rhinosinusitis with and without polyps were enrolled in two categories, A (n=40) and B (n=40) to receive Budesonide and normal saline nasal irrigation respectively. All the patients were evaluated post operatively with Diagnostic Nasal Endoscopy and SNOT 22 Questionnaire for determination of post op wound healing. Key Words: Functional endoscopic sinus surgery, Budesonide, Normal saline, Nasal irrigation, Diagnostic Nasal Endoscopy, SNOT-22
INTRODUCTION The Functional endoscopic sinus surgery (FESS) is one of the most commonly done surgery by otorhinolaryngologist in their day to day practice. Patients diagnosed with chronic rhinosinusitis and Sinonasal polyps intractable to conventional medical treatment undergo FESS in order to restore the ventilation and function of the paranasal sinuses.1 In this surgery, Rigid sinoscope is used to visualize the nase. The sinus openings are identified, opened and the disease is cleared in order to restore normal mucociliary drainage mechanism. The benefits of this surgery is that it is less invasive, provides good surgical field, and thereby decreases post-operative discomfort and complications.2,3 Nearly 80-90% of the patients undergoing FESS have a favourable outcome in terms of symptoms.4-7 Endoscopic surgery is a nasal surgical procedure including the nose and the paranasal sinus for conditions like:
The historical external approach has been explored by FESS and by the year of 2006, the rates of FESS has increased to 0.92 per 1000 Medicare beneficiaries 8. The post-operative period of FESS is crucial as the normal and the diseased mucosa are removed by wound healing and the post-operative care include topical and systemic therapies. Steroids, nasal irrigation, which may be saline or steroid (budesonide, fluticasone, mometasone) and topical antibiotics are included in the topical forms 9. The three fundamental agents in post endoscopic sinus surgery management are:- normal saline, nasal irrigation and topical steroid sprays. The use of Budesonide in various forms such as powder, queous nasal spray or more recently, as budesonide respules in normal saline, as irrigation 9 with high volume, high pressure devices like squeeze bottles is found to be more effective 10. The current practice involves combining aqueous form of Budesonide and nasal saline. The resultant mixture is used as nasal irrigation so as to help in decreasing local inflammation and help in early wound healing and better patient outcomes in terms of symptom relief. Whereas, a prospective study done by Steinke et al.11 in 2009 states that high volume Budesonide for irrigation may improve patients symptoms and CT and endoscopy scores. Volume, dose and frequency of the irrigation was not specified. Similarly, A retrospective study done in 2010 by Nader et al.31 proposed high volume Budesonide irrigation, three times post FESS. 61% of patients had resolution of symptoms. But the study lacked volume and dose of Budesonide to be given. In 2012 Snidvongs et al.13 did a prospective study in post FESS patients by Budesonide irrigation (1mg in 240 ml 4 times). 95% of patients had improvement with Budesonide irrigation. Patients with high tissue eosinophilia had better improvement when compared to patients with low tissue eosinophilia. Patients who had ASA sensitivity, polyposis, asthma had similar improvements compared to those without. Jang et al.14 showed that by giving budesonide nasal irrigation at a dose of 0.5mg in 88mls two times a day to post FESS patients their specific quality of life parameters increased.
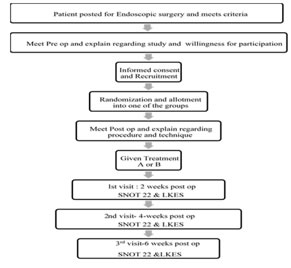
MATERIALS AND METHOD The study was conducted in SRM Medical College Hospital and Research Centre, Kattankulathur’. After the approval by the institutional ethical committee, the study was carried out from 2017 to 2019. INTERVENTIONS: INTERVENTION GROUP: (GROUP A): Budesonide solution (Budesonide respules used for nebulization); 1mg/2ml respules. 1mg budesonide in 400ml normal saline per day. 200ml of the prepared solution is used twice daily, 100ml for each side of nose. COMPARATOR GROUP: (GROUP B): Normal saline (0.9%). 200ml of normal saline twice daily; 100ml each side of nose. DEVICE: Positive pressure high volume squeeze bottle device. For this study the device was standardized to a 200ml squeeze bottle under the commercial name “Nasowash” from ‘Cipla’. ADMINISTRATION: The interventions were administered by the patient using squeeze bottles. The position advised was bending down position over a sink/basin and patient inserting the tip of the squeeze bottle into a nostril and pressing the bottle and irrigating each nose with 100ml of the solution and allowing the run off to flow out. OUTCOMES: PRIMARY OBJECTIVES: Efficacy of the two arms compared by: SNOT 22 score (3 post-operative visits) Lund – Kennedy Endoscopic score (3 post-operative visits) POST OPERATIVE VISITS: 3 post-operative visits were done. First visit at 2 weeks post op. The second visit was at 4 weeks post op and 3rd visit at 6 weeks post op. During each of those visits, the ‘patient was asked to fill the SNOT-22 questionnaire and endoscopic Lund-Kennedy score was then assessed by the principal investigator’. In the event the patient was not able to come for follow up, then in such cases the SNOT 22 questionnaire was completed over mail or telephonic interview. In such cases the endoscopic LK score could not be assessed.
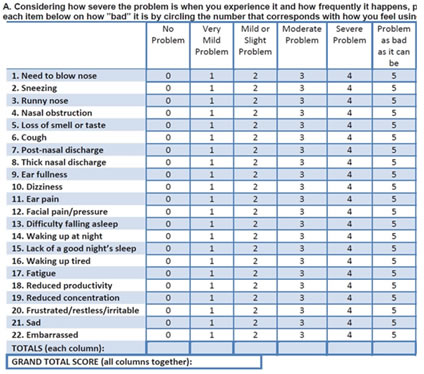
SNOT 22 SCORE: (“SINO-NASAL OUTCOME TEST”) ‘SNOT 22 is a standard questionnaire consisting of 22 symptoms’ related to nasal pathology and its associations which can be an indicator of the disease burden for the patient pre operatively, and when used post operatively, can be used to analyse the improvement in disease symptoms following the intervention. Each of the 22 symptoms have a score of 0-5 based on the severity and total score is out of 120.
LUND KENNEDY ENDOSCOPIC SCORE: The Lund-Kennedy endoscopic score is an objective endoscopic assessment done by the endoscopist. It has 3 components, each with a score of 0-2 and total score is 7.
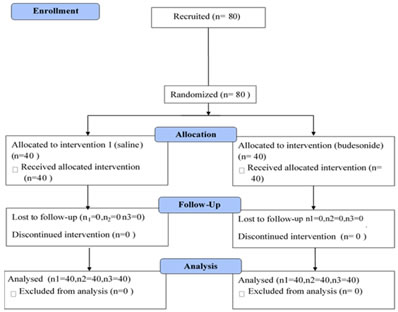
SAMPLE SIZE: Study used to calculate sample size: “Hartwig S, Linden M, Laurent C, et al... Budesonide nasal spray as prophylactic treatment after polypectomy (a double blind clinical trial). J Laryngol Otol 102:148–151”, 1988(66) Power of study: 80% Significance level: 95% Sample size was calculated to be an estimated 44 patients in each arm Formula used to calculate sample size n= (s1+s2)2 x [(z1-a/2) + (z1-b/2)]2 / [x1-x2]2 RANDOMIZATION: Method of randomization: Randomization was done by “Random allocation software (Version 1.0 May 2004) [Random allocation software has been developed by M.Saghaei MD., Department of Anesthesia, Isfahan University of Medical Sciences”, The sequence generation was done by an independent resident’. Method of allocation concealment: Sealed envelope that will be opened only at the time of allocation after randomization, to which the investigator is blinded. Implementation: Eligible patients were recruited by the principal investigator. Recruited patients were randomized by sealed envelope by a designated staff nurse who dispensed the medications according to the assigned groups. Blinding: Double blind study. The investigator is blinded as to which patient receives which treatment. This is ensured that after randomization, the patient is given the sealed envelope which is opened only by the nurse in charge of dispensing the medication, in the absence of the investigator. The patient is blinded to which group he belongs to as both groups receive normal saline. One group will receive budesonide solution in an air tight container from which they have to prepare the douching solution daily. The other group will receive an identical colourless saline solution in an identical container that they have to add to the irrigation. Statistical methods: Baseline data comparisons would be made using descriptive statistical methods such as mean, standard deviation etc. The continuous variables would be compared by using independent ‘student-t test’. ‘Binary variables would be compared using Chi-square test’. 95% confidence interval would also be calculated. METHEDOLOGY: RESULTS
n1 = first assessment; n2 = second assessment; n3= third assessment PRIMARY OUTCOME: FIRST ASSESMENT: SNOT SCORE:1
The BUDESONIDE group had a significantly better statistical data compared to the SALINE group. LUND-KENNEDY SCORE:1
The budesonide group had significantly better statistical data compared to the SALINE group.
SECOND ASSESMENT: SNOT SCORE:2
During the second visit the SNOT scores of BUDESONIDE group was better compared to the SALINE group
LUND-KENNEDY SCORE:2
The budesonide group of patients endoscopic scores were statistically superior to that of saline group.
THIRD ASSESMENT: SNOT SCORE:3
The final assessment of the patients revealed that the SNOT score of BUDESONIDE group was better than that of SALINE group. LUND-KENNEDY SCORE:3
Comparing the LUND-KENNEDY scores of both the group during the final assessment it is evident that the BUDESONIDE group patients had a better result compared with SALINE group.
DISCUSSION Topical therapy has become vital in the management of post endoscopic sinus surgery patients. The current gold standard of practice is ‘normal saline nasal irrigation and topical steroid spray’. Normal saline nasal irrigation has mainly mechanical effects to the post-operative sinus cavities while topical steroid sprays have pharmaceutical action on the sinus cavity mucosa. But as mentioned previously, steroid sprays being a low volume low pressure method, has considerably less distribution in sinuses than high volume positive pressure devices. Hence the use of budesonide nasal irrigation, which combines both the saline and topical steroid part is a promising method. Even though the use of high-volume budesonide irrigation in saline is promising theoretically, it is not widely used. The safety and efficacy of budesonide high volume irrigation needs research before being prescribed regularly. The safety of budesonide nasal irrigations has been studied by Bhalla et al..(133) and Welch et al..(134) studying 1mg budesonide/day for 8 weeks and 2mg budesonide/day for 8 weeks respectively and has reported no suppression of HPA axis or any adverse effects related to budesonide usage. The studies regarding efficacy of budesonide nasal irrigations in post endoscopic sinus surgery patients are few and inconclusive, with majority of them, barring one being level 4 evidence. Steinke et al..11 did a prospective pilot study on 8 chronic hyperplastic eosinophilic sinusitis patients who had not been operated and found improvement in CT and symptom scores. But this study observed a very small number of “patients who had not undergone endoscopic sinus surgery”. Nader “et al.12 did a study on patients” diagnosed with CRS who are not amenable to “medical and surgical management” and observed that the effect of high volume budesonide irrigations in such patients. The exact dose and volume of budesonide was not mentioned. They observed that 61% of patients had resolution of symptoms. This study observed the effect of high-volume budesonide in treatment refractory patients but not in patients routinely after ESS. Snidvongs et al.13 did a study on 111 CRS who underwent ESS. They received either budesonide 1mg in 240ml or betamethasone. They observed that there was a significant ‘improvement in symptom score, SNOT 22 score and endoscopy score following 3 months’ usage of budesonide nasal irrigation. But as there was no control arm comparing the efficacy with the current standard of practice – normal saline irrigation with nasal sprays, there cannot be a direct comparison of the efficacy between the two modalities of intervention. Jang et al.14 did a study on 60 patients who had been prescribed budesonide nasal irrigation but who lapsed using it for at least 1 month in between and compared the SNOT 20 and LK endoscopy scores from when the patients were using budesonide nasal irrigation, to when they lapsed. They found that the scores were significantly better when the patients were using budesonide nasal irrigation. Kang et al.(138) did a study on 12 CRS patients with bronchial asthma following ESS using high volume budesonide irrigations. They found that there was significant betterment in the SNOT 22 and endoscopy scores in patients following budesonide irrigation. Also they observed that by using budesonide nasal irrigations, dosage of oral steroids was also able to be reduced. Kosugi et al.(139) did a prospective study on 16 CRS patients who underwent ESS who did not respond to topical steroid nasal spray therapy. They gave 0.5mg budesonide per day as high volume irrigations and observed that 75% of patients had good improvement of SNOT 22 and endoscopy scores. The only level I evidence on budesonide nasal irrigation is a study done by Rotenberg et al. ‘in 60 patients with Samter’s triad who had undergone ESS’. They undertook a RCT comprising of 3 groups – one that received budesonide nasal irrigation (1mg in 240ml per day), second group which received ‘saline nasal irrigation with budesonide nasal spray’ and third group with normal saline nasal irrigation alone. They found that ‘there significant improvement in SNOT 22 and Lund-Kennedy endoscopic scores within each group following the intervention at 6months and 1 year post surgery. But there was no statistically significant difference in scores when comparing the 3 groups and hence they arrived at a conclusion that budesonide high volume nasal irrigation was not superior to normal saline irrigation. The caveat with this study was that it was done in patients with Samter’s triad and hence not in patients with a classic CRS or nasal pathology which could explain the difference in outcome when compared to our current’ study. Thus, according to present knowledge it can be concluded that though “high volume budesonide nasal irrigations” have been found to be beneficial, its efficacy yet to be compared to the standard of care in a controlled trial. Hence our study aims to address this deficiency in our current knowledge about budesonide nasal irrigation.
CONCLUSION Budesonide nasal irrigation with positive pressure high volume device has been found to be more efficacious than normal saline nasal irrigation in post FESS patients. Hence in future management protocols and guidelines, budesonide may be included as a replacement for normal saline nasal irrigation.
ACKNOWLEDGEMENT- I would like to express my deep and sincere gratitude and thankfulness to all my teachers, parents and friends for their guidance, encouragement and support.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.