 Home
Home
|
Table of Content - Volume 18 Issue 3 - June 2021
Deviated nasal septum and its association with chronic maxillary sinusitis
Jitendra K Rathod1, Swati J Rathod2*
{1Associate Professor, Department of ENT} {2Assistant Professor, Department of Dentistry} M.G.M. Medical College and Hospital, Aurangabad, Maharashtra, INDIA. Email: drswatirathod30@gmail.com
Abstract Background: Deviated nasal septum is a very common finding in ENT clinic, most of the times, as incidental findings without any related symptom. Sometimes it present in association with suspiciously related sinusitis. Our study is to identify the possible association between deviated nasal septum and maxillary sinusitis. Methods: A prospective observational study. The standard procedure of examination of ear, nose, throat, oral, face and neck was carried out on each patient. Deviated nasal septum was diagnosed after detailed history and meticulous examination of nose. After clinical examination all cases were screened for maxillary sinusitis using roentgenographic evaluation of paranasal sinuses. Results: This study comprises of 300 patients attending our outpatient department of ENT. We studied 300 patients, 210 males and 90 females, The highest incidence of deviated nasal septum was in age group 21 to 30 years (38%). The youngest patient recorded is 8 years, while oldest is 60 years. (Table 1). The present study revealed higher incidence of deviated nasal septum in males (70%) than females (30%) with ratio of 2.33:1. The highest incidence of deviated nasal septum is 'C' shaped is 82%, While 'S' shaped is 2%, spur is 14% and Anterior deviation is 2%. The commonest symptom was nasal obstruction in 64% which was unilateral in 54% cases and 10% bilaterally. Next common complaint was frequent attacks of common cold in 52% of cases and recurrent headaches in 44%. 4. 8% of cases had Nasal discharge. While 4% had Nasal deformity, 4% cases had mouth breathing, 2% cases had epistaxis and 2% cases loss of smell. Maxillary sinus was involved in 62% of cases. It was noted that the maxillary sinus on same side and opposite side to that of septal deviation was involved in 10% and bilateral sinusitis was observed in 42% of cases. Conclusions: According to our finding, there is significant association observed between deviated nasal and maxillary sinusitis. Attributing sinuses disease to deviated nasal septum may lead to over treatment of the patient and unnecessary surgery. Keywords: Deviated septum, Sinusitis, mouth breathing, epistaxis.
INTRODUCTION The nasal septum is an important functional and aesthetic structure of the nose. It is responsible for regulating airflow through the nose while lending shape and support to the nose.1 Deviated nasal septum (NSD) can be described as an asymmetry of the nasal septum. Both traumatic deviation and growth-associated abnormalities of the nasal septum may lead to significant airway obstruction and also cosmetic deformity.2 Paranasal sinuses (PNS) are the air containing spaces in skull. They helps to lighten the skull, perform the function of humidification of air and provide resonance to voice.3 Deviated nasal septum is most common cause of maxillary sinusitis. Deviated nasal septum produces nasal obstruction, which obstruct the ostia of the sinus and also ostia that are located high on the superomedial wall. Also this is a poor location for natural drainage of the sinus especially when the mucous membrane is congested. The ostia are obstructed resulting in the stagnation of secretion in the sinus and infection follows. This being a relatively common condition, it was decided to study at least 300 cases of deviated nasal septum and to correlate its association with maxillary sinusitis. MATERIALS AND METHODS This study comprises of 300 patients attending our out patient department of ENT, MGM Medical College and hospital, Aurangabad. All cases were studied prospectively to obtain data. All patients selected with deviated nasal septum after carefully excluding all cases with history of trauma, any intra or extra nasal surgery, intra or extra nasal malignancy, nasopharyngeal irradiation or any associated nasal pathology. A detailed history of his/her complaints was taken under the various headings mentioned in the proforma. The standard procedure of examination of ear, nose, throat, oral, face and neck was carried out on each patient. Deviated nasal septum was diagnosed after detailed history and meticulous examination of nose. After clinical examination all cases were screened for maxillary sinusitis using roentgenographic evaluation of paranasal sinuses
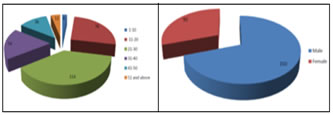
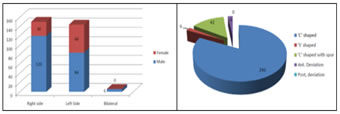
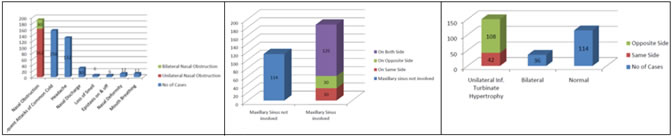
OBSERVATION AND RESULTS All the patients who attended the E.N.T. OPD were thoroughly examined and out of these cases of deviated nasal septum are being reported here, in whom the symptoms were attributed to the septal deviation. The highest incidence of deviated nasal septum was in age group 21 to 30 years (38%). The youngest patient recorded is 8 years, while oldest is 60 years. (Figure 1).The present study revealed higher incidence of deviated nasal septum in males (70%) than females (30%) with ratio of 2.33:1(Figure 2) Both the left and right sided deviation were present in both sex, male predominating in both types of deviation. The deviation towards right was commoner of the two being present in 50%, while 48% of the patients showed deviation towards left and 2% presented bilaterally. (Figure 3) In the present study various types of deviated nasal septum had revealed. The highest incidence of deviated nasal septum is 'C' shaped is 82%, While 'S' shaped is 2%, spur is 14% and Anterior deviation is 2%. (Figure 4) The different complaint of patient suffering from deviated nasal septum in order of frequency was recorded. The commonest symptom was nasal obstruction in 64% which was unilateral in 54% cases and 10% bilaterally. Next common complaint was frequent attacks of common cold in 52% of cases and recurrent headaches in 44%. 4. 8% of cases had Nasal discharge. While 4% had Nasal deformity, 4% cases had mouth breathing, 2% cases had epistaxis and 2% cases loss of smell. (Figure 5) Maxillary sinus was involved in 62% of cases. It was noted that the maxillary sinus on same side and opposite side to that of septal deviation was involved in 10% and bilateral sinusitis was observed in 42% of cases. (Figure 6) The present study revealed that in 50% of the cases have unilateral inferior turbinate hypertrophy and in which 36% cases showing opposite side hypertrophy and only 14% cases showing same side inferior turbinate hypertrophy.12% cases showing bilateral inferior turbinate hypertrophy.38% showing normal appearance of inferior turbinate. (Figure 7). Figure 1 Figure 2 Figure 3 Figure 4 Figure 5 Figure 6 Figure 7 Figure 1: The incidence of deviated nasal septum; Figure 2: Shows higher incidence of deviated nasal septum in males (70%) than females (30%) with ratio of 2.33:1; Figure 3: Shows sex and side relationship; Figure 4: Shows the different types of deviated nasal septum; Figure 5: Shows various symptoms in order of frequency; Figure 6: Shows maxillary sinus affection in the cases of deviated nasal septum; Figure 7: Showing the inferior turbinate hypertrophy in cases of deviated nasal septum
DISCUSSION The patient complaining of a blocked nose is an extremely common presentation in the Otorhinolaryngology out patient department and one of the important diagnostic possibilities includes deviated nasal septum. Among the local causes which can produce obstruction in nose, nasal septal deformity is most important which either directly initiates a disturbance in the physiology of nose or can aggravate to severity of other nasal symptoms. The symptoms, associated with deviated nasal septum are as difficulties in breathing though the nose, nasal congestions, sinus infections, nosebleeds, sleep problems, headache, and postnasal drip.4 5Various etiology factors may contribute for the development of deviated nasal septum which can be classified as congenital, genetic effects causing aberrant growth, trauma, infection, or nasal cavity neoplasms. 6 7 The present study was done on 300 selected cases of deviated nasal septum. Only those cases were included in whom the symptoms were attributable to the septal deformity. Special attention was paid to maxillary sinus affection, so as to establish the role of deviated nasal septum in causation of maxillary sinusitis. The diagnosis of maxillary sinusitis was made on the basis of roentgenographic evaluation of paranasal sinuses. The earlier workers have reported a definite incidence of deviated nasal septum, suggesting thereby that straight septa could be seen in many. But still most of the authors claim that it is rare for the nasal septum to be absolutely in midline. This view received slight modification and it was stated the posterior border of nasal septum is never deviated, no matter how severe the deflection is present in the anterior part (Gray 1978; Scott, 1956). 8 9 It seems that the focus of attention in the recent studies have been shown towards finding out the incidence of deviated nasal septum in the general population. This possibility suggests that majority of the authors believed that the septal deviation may be considered to be present in all but it gains significance only when it is severe enough to cause disturbance in the physiology of nose and becomes symptomatic. In the present study the higher incidence found in age group of 21-30 years. The youngest patient recorded is of 8 years, while oldest is 60 years. This can be compared to a study done by Poore and Gupta. 10 The present study revealed that septal deformities are more common in males 70% than in female 30% ratio being 2.33:1 (M/F) which can be compared with the study done by Shoib et al. In which there were 112 males and 88 females showing a male predominance.11 In the present study males showed higher incidences (40%) of Septal deviation on right side and (28%) in left side (total is 68%) while deviation was on left side in male (10%) and (20%) in females on left sides and both side only 2% in males. In the study by Clark G. Wallace C: (1970) the sex ratio for the right sided deviation was 1.2:1 (M:F) and that for left side deviations was 10.5:1(M:F), thereby showing that right sided deviations were more common in females as compared to males. 12 The above mentioned sex ratio could be explained on the basis of the fact that deviation of septum is in itself more common in males than females and this preponderance is well maintained when the side of deviation is considered. In the present study all the nasal and extranasal symptoms presented in cases of deviated nasal septum. The various symptoms pertaining to nose were nasal obstructions in 64%, frequent attacks of common cold 52%, headache 44%, nasal discharge 10%, nasal deformity 4%, mouth breathing 4%, epistaxis 2% and loss of smell 2%. Nasal obstruction was felt on the side of deviation of septum and on the side of concavity because of hypertrophied turbinates. The study was done by Shoib et al. headache was seen in 186 patients (93%), nasal obstruction in 178 patients (89%), nasal discharge in 126 patients (63%), facial pain in 95 patients (47.5%), fever in 55 patients (27.5%), halitosis in 20 patients (10%), cough in 17 patients (8.5%), fatigue in 6 patients (3%). 11In the study conducted by Singh headache was the predominant symptom seen in 80% of patients, nasal blockage was seen in 76.66%, nasal discharge in 43.33%, facial pain in 40% patients.13 Majority of cases in the present study showed C type of deviation 82% and 2% as S shaped. Spurs found in 14% of cases 2% of case showed anterior deviation. Similar types of deformity described by shoeb et al. and Jadia S. et al.11,14 In the present study maxillary sinus was found affected in 62% cases, in which on the side of deflection in 10% cases, on the concave side of septal deviation is also 10% cases, bilateral involvement of maxillary sinus was present in 42% cases. It is clear from our findings that bilateral involvement of maxillary sinus was of greater frequency than the side of deptal deviation and also opposite of septal deviation. It is also clear from our findings that maxillary sinus on the side of septal deviation and opposite side of septal deviation was affected in equal frequency. In correlation with the same it is to be noted that the septal deviation in majority of cases were towards right side. On the whole it may be concluded that the maxillary sinusitis was found in 62% of cases in the present series, which in itself is a higher percentage as compared to the incidence of maxillary sinusitis in general. Therefore it can be concluded that deviated septum definitely produces definite predisposition to the maxillary sinusitis
SUMMARY AND CONCLUSION The present study revealed following facts-
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.