 Home
Home
|
Table of Content - Volume 19 Issue 3 - September 2021
A clinico-epidemiological study of hearing loss in adult patients presenting to a tertiary healthcare center in India
Shwetha1*, Sathyaki D C2, Pancham Ponnana3
1Associate Professor, 2Assistant Professor, 3Audiologist, Department of Otorhinolaryngology, Head and Neck Surgery, Kodagu Institute of Medical Sciences, Madikeri, INDIA. Email: shwetha2210@gmail.com, sathyaki_dc@yahoo.co.in, panchamponnana@gmail.com
Abstract Background: The objectives of the study are: 1. To determine the profile of patients presenting with hearing loss. 2. To determine the causes of hearing loss in adult patients of various age groups. The cases for the study comprised of adult patients aged >/=20years, presenting to the ENT Out-patient Department with complaint of hearing loss. Detailed history thorough ENT examination including Examination of the ear, nose and throat with Bull’s eye lamp, Otoscopic/Otomicroscopic/Otoendoscopic examination with photo-documentation of the ear status when required, tuning fork tests, and a battery of audiological tests including pure-tone audiometry, impedance audiometry and Brain-stem Evoked Response audiometry (when required) were conducted and the reports of the same were enclosed with the Pro forma of the patients. Results and Discussion: Hearing loss is more common in old age and more male patients presented with hearing loss. The most common symptom seen with hearing loss was tinnitus which was commonly ringing type and this was commonly seen in older patients associated with sensori-neural hearing loss. The most common type of hearing loss was sensori-neural hearing loss seen more commonly in older patients and associated with tinnitus. The definitive diagnosis for patients with sensori-neural hearing loss was difficult to specify with the most common diagnosis being presbyacusis, followed by noise induced hearing loss. The second common diagnosis was Chronic Otitis Media(COM). Key Word: hearing loss.
INTRODUCTION What differentiates a human being from other species is the ability to express ideas and concepts by means of language, the acquisition of which is dependent on normal hearing. Hearing is arguably one of the most important special senses for man. Hearing loss can vary from mild to profound resulting in poor quality of life or at the other end causing severe disability. Deafness is one of the most significant disabilities noted in our country. It is the second most common cause of disability in India. According to national data, nearly 63 million people (6.3%) in our country suffer from significant auditory loss.1 Hearing loss could be a very distressing symptom. It causes developmental difficulties in children and communication difficulties in adults. These all have a major impact on quality of life and work efficacy leading to cognitive and emotional problems.2,3,4 It also increases the burden on the health care system and society both causing an adverse effect on health and survival. 5,6 In the legislature of India, deafness is defined as:
There are several causes of hearing loss, some of which are preventable. Hearing loss can be classified as conductive, sensori-neural or mixed type. In most cases the conductive type of hearing loss can be prevented. In India, conductive hearing loss is still common and this needs to be addressed as this is a preventable or curable cause of hearing loss and also the associated symptoms such as ear discharge and tinnitus affect the quality of life. Some patients who present with chronic otitis media and foul-smelling discharge find social acceptance a challenge due to the associated foul smell of the discharge. A proper surgery will address the issue of ear discharge as well as the hearing and in many parts of our country patients still do not have an access to this kind of health care. Also, increasing exposure to noise needs to be addressed, as the consequences of the same go unnoticed. Our youth are exposing themselves to loud sounds with the use of personal listening devices (ear phones and head-phones), the consequence of these remains to be established.
OBJECTIVES 1. To determine the profile of patients presenting with hearing loss. 2. To determine the causes of hearing loss in adult patients of various age groups.
METHODS The study was carried out in the Department of ENT, Kodagu Institute of Medical Sciences, after obtaining the Institutional Ethical Committee clearance. A written informed consent was obtained from all patients participating in the study. The cases for the study comprised of adult patients aged >/=20years, presenting to the ENT Out-patient Department with complaint of hearing loss between June 2017 and December 2018. A total of 1134 adult patients presented with hearing loss, of which 1020 who gave consent were included in the study. Detailed history, thorough ENT examination including Examination of the ear, nose and throat with head-light, Otoscopic/Otomicroscopic/Otoendoscopic examination with photo-documentation of the ear status when required, tuning fork tests, and a battery of audiological tests including pure-tone audiometry, impedance audiometry and Brain-stem Evoked Response audiometry (when required) were conducted and the reports of the same were enclosed with the Pro forma of the patients. In patients presenting with Ear wax or debris in the EAC the same was cleared following which the patient was subjected to audiometric tests. The patients were also subjected to thorough systemic examination and blood investigations when required to rule out systemic causes. The audiometry tests were conducted in a sound-proof room by a certified audiologist. Data was collected in a standard pro forma and the audiometry reports were enclosed with each pro forma.
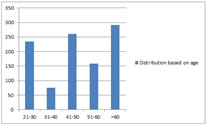
RESULTS AND DISCUSSION Figure 1: Distribution based on age
Figure 2: Sex
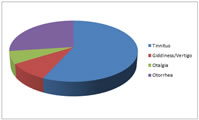
Figure 3: Associated symptoms
Figure 4: Type of Hearing loss It can be seen from the results that the hearing loss in adults is more common in old age and also more male patients presented with hearing loss. Thus the most common symptom seen with hearing loss was tinnitus which was commonly ringing type and this was commonly seen in older patients associated with sensori-neural hearing loss. Some patients who presented with hearing loss and tinnitus had exposure to noise, 12 patients were from the armed forces who had hearing loss associated with tinnitus. Also, we had an anesthetist whose SNHL pattern corresponded to noise exposure type. The second most common symptom was ear discharge and this is seen more commonly in the younger age group in the study. The most common type of hearing loss was sensori-neural hearing loss seen more commonly in older patients and associated with tinnitus. The definitive diagnosis for patients with sensori-neural hearing loss was difficult to specify with the most common diagnosis being presbyacusis, followed by noise induced hearing loss. The second common diagnosis was Chronic Otitis Media(COM). Patients with COM had central perforation commonly with marginal perforation seen in only 4%. 16 patients who had acute otitis media, presented with hearing loss. 13 patients with acute trauma to the ear with hearing loss had minimal to mild conductive hearing loss, showed rupture of the tympanic membrane. Only 2 patients had sensori-neural hearing loss on one side and Conductive pathology in the other ear, rest of them always had a mixed hearing loss.
CONCLUSION The study indicates the reducing pattern of conductive hearing loss and increased sensorineural hearing loss in the Indian scenario. The increased sensori-neural hearing loss may be due to the increased exposure to noise and the increased age of survival. However the prevalence of preventive causes of conductive hearing loss such as chronic otitis media and serous otitis media still persist indicating that proper treatment can reduce this cause of hearing loss. It can also be noted that treating the elderly patients for hearing loss with hearing aids becomes difficult when they have perforations in the tympanic membrane. This needs to be addressed at an earlier stage in their life. Health education and the benefits of ear protection device usage in reducing noise induced hearing loss should be stressed to reduce the impact of noise on hearing loss. Further occupational exposure to noise needs to be addressed not just in the factories and industries but also in professionals like the army and other professionals including doctors working continuously in ICUs who are also exposed to the continuous sounds of monitors in ICU.
SUMMARY What differentiates a human being from other species is the ability to express ideas and concepts by means of language, the acquisition of which is dependent on normal hearing. Hearing is arguably one of the most important special senses for man. Hearing loss can vary from mild to profound resulting in poor quality of life or at the other end causing severe disability.
REFERENCES
Policy for Articles with Open Access
|
|


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.