 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 8 Issue 2 - November2018
Histopathological lesions of nose, paranasal sinuses and nasopharynx at a tertiary care centre
A A Vare1*, R A Vare2, B Gurme3
1Associate Professor, 2Post Graduate Student, Department of Pathology, MGM Medical College and Hospital, 431003 Aurangabad, Maharashtra, INDIA. 2Professor and HOD, Department of ENT, MGM Medical College and Hospital, 431003 Aurangabad, Maharashtra, INDIA. Email: vareanil11@gmail.com, reenavare@gmail.com , bhagyashrigurme10@gmail.com
Abstract Aims and Objectives: 1To study the incidence of various lesions of nasal cavity, nasopharynx and paranasal sinuses. To study site wise incidence of different Non-neoplastic and Neoplastic lesions of nasal cavity, nasopharynx and paranasal sinuses 3To compare the results with the available data. Material and Methods The present study was carried out on 45 cases of lesions of nasal cavity, nasopharynx and paranasal sinuses who came to ENT department during September 2016 to September 2018 and study was carried out at pathology department, MGM Medical College, Aurangabad. 2Inclusion Criteria: Patients came to ENT department (OPD and IPD) with non-neoplastic and neoplastic lesions of nose, paranasal sinuses and nasopharynx. 3All the specimens were preserved in 10 % formalin and number of sections was taken from different sites according to the size of the specimen. In cases of small biopsies whole specimen was taken. 4All sections were studied by routine paraffin sectioning and Haematoxylin and eosin stain. Special staining by PAS and masson’strichrome were undertaken whenever applicable. Results: In present study of 45 cases, 25 were diagnosed as non-neoplastic (18-inflammatory polyps, 2 - fungal origin and 5 -non-specific inflammatory lesions) and 20 were diagnosed as neoplastic lesions (14-benign and 6- malignant lesions) Conclusion: It is important to recognize the range of non-neoplastic lesions in this region and to differentiate them from neoplastic lesions because of different treatment modality and emotional burden on the patient. Thus, the present study was carried out to record the various neoplastic and non-neoplastic lesions of nasal cavity, paranasal sinuses and nasopharynx on the basis of age, sex, site wise distribution. Key Word: Benign, Malignant, Nose, Nasopharnx, Non-neoplastic, Paranasal sinus.
INTRODUCTION The parts of the upper respiratory tract included in our study are: Nasal cavity, Paranasal sinuses and Nasopharynx. The nasal cavity, paranasal sinuses and nasopharynx form functional unit of nose and is principally involved in filtering, humidifying and adjusting the temperature of inspired air.1 Sinonasal tract and nasopharyngeal lesions can be non-neoplastic (polyps, bacterial and fungal infections) and neoplastic (benign and malignant).2 The presenting features, symptomatology and advanced imaging technique help to reach a presumptive diagnosis, but histopathological examination remains the mainstay of final definitive diagnosis. Thus, careful histological workup is essential for a correct diagnosis and timely intervention.2 Polypoidal mass in the nose is a very common lesion encountered in clinical practice. It may be due to the most frequently occurring simple nasal polyp or polypoidal lesions due to a variety of other pathologic entity ranging from infective granulomatous diseases to polypoidal neoplasm including malignant ones.3 Nasal obstruction is the most common symptom. Other symptoms include nasal discharge, epistaxis and disturbances of smell.4 The present study was carried to study the age and sex distribution of nose, paranasal sinus and nasopharynx, their clinical presentation and to categorize them histopathologically.
MATERIALS AND METHODS The present study was carried out on 45 cases of lesions of nasal cavity, nasopharynx and paranasal sinuses who came to ENT department during September 2016 to September 2018 and study was carried out at pathology department, MGM Medical College, Aurangabad. The biopsies and the specimens were received in 10% formalin along with clinical data. The specimens which requires fixation were fixed in 10% formalin for 24 hours after noting the gross morphological features. Sections were stained with Hematoxylin and Eosin (HandE) stain. Special stains like Periodic Acid Schiff, Ziehl-Neelson, Masson’s trichrome etc were used wherever necessary. The stained sections were studied under light microscopy. The procedures for processing and staining of tissue given in Cellular Pathology Techniques, 4th edition by C.F.A. Culling, 1985 and Theory and Practice of Histological Techniques by Bancroft and Gamble, 2002168 were followed.
OBSERVATION AND RESULT The present study includes total 45 cases of non-neoplastic and neoplastic lesions of nasal cavity, paranasal sinuses and nasopharynx during the period of September 2016 to September 2018. All the cases of lesions of nasal cavity, paranasal sinuses and nasopharynx from ENT department (OPD and IPD), MGM medical college and hospital are included in our study during above mentioned period. We have totaled 45 such cases, out of which 25 are non-neoplastic and 20 are neoplastic. Out of 20 neoplastic lesions, 14are benign and 6 are malignant.
Table 1: Incidence Of Neoplastic And Non-Neoplastic Lesions
From table 1, it is seen that non-neoplastic lesions are commoner than neoplastic lesions in the nasal cavity, paranasal sinuses and nasopharynx. Benign lesions are more in number than the malignant lesions in our study.
Table 2: Site distribution of neoplastic and non-neoplastic lesions
Table 3: Histological diagnosis of Non-neoplastic, Benign and Malignant lesions
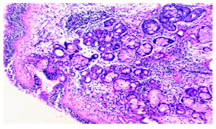
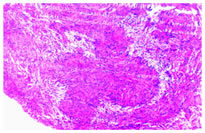
Age Distribution neoplastic and non-neoplastic lesion In our study, non-neoplastic lesions and malignant lesions are commonly found in 7th and 8 th decade of life. Benign lesions are more commonly found in 2nd, 3rd and 4th decade of life. Sex distribution of neoplastic and non-neoplastic lesion: In our study, non-neoplastic lesions are male predominant, benign lesions are equally distributed in both the sexes and malignant lesions are mostly found in female population. DISCUSSION Tumours of nasal cavity, paranasal sinuses and nasopharynx are uncommon and constitute only 0.3% of all malignancies. In our study of the 45 cases, 25 were non-neoplastic and 20 were neoplastic lesions forming a ratio of non-neoplastic to neoplastic lesions as 1.25: 1 and the ratio of benign neoplastic to malignant lesions as 2.3: 1. In our study, sinonasal masses had slight predeliction for female emonstrating M:F of 1:1.04 similar to study by Bakari et al5 and parajuli and Tuladhar6 i.e. 1:1.12 and 1:1.13 while the study by Trilok et al7 revealed an opposite ratio showing male preodominance i.e. 1.69:1. In our study Second to Seventh decade of life are most vulnerable period for development of sinonasal masses.In our study there are 55.5% non-neoplastic lesions and 44.4% neoplstic lesions which is close to incidence observed by Khan et al.8 Non-Neoplastic Lesions Nasal polyp: In present study, Nasal polyp was the most common lesion , constituting 72%( 18 cases) of all non-neoplastic lesions, which was close to the incidence observed by Bhattacharya J et al (2015)2 i.e. 73.4%. In the present study, male to female ratio was 1.57:1 for nasal polyp which is similar to study by Zafar et al (2008)9. In present study, the age of presentation ranged from 11-70 years of age but peak incidence was noted in 2nd, 3rd and 4 th decade of life. Figure 1: Inflammatory polyp 10x
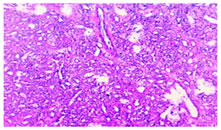
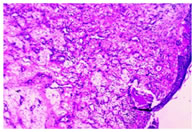
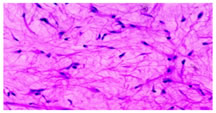
Non specific inflammatory lesions-The study included 5 cases of non-specific inflammatory lesion, constituting 20% of non-neoplastic cases. Fungal lesions: In present study we diagnosed two cases of fungal infections, both were occurring in nasal cavity. In the present study, mucormycosis constituted 4% of all non- neoplastic lesions. Alpesh M. Maru et al10 also observed 4% incidence of mucormycosis. Benign Neoplastic Lesions Benign fibrous histiocytoma: It was found that the incidence of benign fibrous histiocytoma in the present study was 7.14%, which was 2.3% in study by Dasgupta et al (1997)3. Hemangioma: Among 14 cases of benign lesion we observed 5 cases of hemangioma. Out of 5 cases 4 are capillary hemangioma and 1 is of cavernous hemangioma. So we found capillary hemangioma as predominant type. It is seen that the incidence of hemangioma in the present study is 35.71%.This was close to the incidence observed by Aparna M et al.11 i.e. 38.46. In our study, all cases of hemangioma were in the nasal cavity with female preponderance. Figure 2: Capillary hemangioma10x Angiofibroma: The incidence of Angiofibroma in the present study is 21.4%. This was close to incidence observed by Dasgupta et al (1997)3. There was male preponderance in our study. In our study, two cases were in the nasal cavity, one case is from nasopharynx. According to Khan et al (2006)8 all the cases were found in nasopharynx with profuse and recurrent epistaxis from the polypoidal mass as the chief complaints.
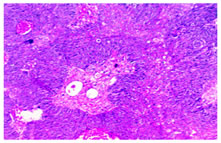
Figure 3: Angiofibroma 10x
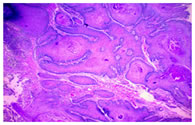
Inverted papilloma: In the present study, there was 1 case (7.14%) of inverted papillomas and patient was 66 years female. In a study by Dasgupta et al3, inverted papilloma was reported in 5 cases (3.9%) and commonly seen in third to sixth decade. In our study, one of the case, 71 years male complaining with left nasal mass and obstruction, showed inverted sinonasal papilloma leading to verrucous carcinoma. Lesperance et al (1995) had reported 27% malignant transformation in inverted papilloma.12
Figure 4: Inverted papilloma leading to verrucous carcinoma 4x
Schwannoma: The incidence of Schwannoma in the present study is 14.2% which is higher than the study by Aparna M et al (2012)11 i.e.7.69%. Male to female ratio was 1:1 in our study. Figure 5: Schwannoma 10x
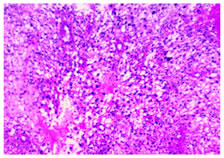
Maxillary Myxoma: In present study we found one case 18 year male, presented with right cheek swelling diagnosed as maxillary myxoma which constitutes 7.14%. Our case was found in right maxillary sinus.Ghosh et al in 1973 reported 10 cases of myxomas, 6 in mandible and 4 in maxilla13. Figure 6: Maxillary Myxoma40x Malignant Neoplastic Lesion Squamous cell carcinoma: It is seen that the incidence of squamous cell carcinoma inthe present study is 83.33% which was higher than study by Dhillon, et al. (2016)14 i.e.71.4% and study by Thakur et al (2001)15 i. e.67.50%. It is evident that there is female preponderance in our study. Falguni shah et al16 also observed female preponderance. In other studies, there was male preponderance. Out of 5 cases, 4 were occurred in nasal cavity and one was in paranasal sinus. In study by GretheHarbo et al (1997)17, squamous cell carcinoma was predominantly occurred in paranasal sinus. In our study we found the cases of squamous cell carcinoma in 7th and 8 th decade of life. Sarcoma: The incidence of sarcoma in the present study was 16.66 % (one case found in nasal cavity), which was 3% in study by GretheHarbo et al (1997)17. According to GretheHarbo et al (1997) maximum numbers of cases were found in paranasal sinuses than nasal cavity. Figure 7: Moderately differentiatedsquamous cell carcinoma 10x
Figure 8: High grade sarcoma 10x CONCLUSION From our study it is evident that the polypoidal masses in the nasal cavity paranasal sinuses and nasopharynx form a complex of lesions ranging from the non-neoplastic inflammatory lesions to benign and malignant neoplasms with a spectrum of histopathologic findings and affect all the ages.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.