 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 8 Issue 2 - November 2018
A descriptive study of injuries among fatal road traffic accidents
Shaik Khaja Moinuddin1, S Mohan Singh2*
1Associate Professor, Department of Forensic and Toxicology, Osmania Medical College, Hyderabad, Telangana, INDIA. 2*Associate Professor, Department of Forensic and Toxicology, Kakatiya Medical College, Warangal, Telangana, INDIA. Email: dr.s.mohansingh@gmail.com
Abstract Road traffic accidents (RTAs) are increasing with rapid pace and presently these are one of the leading causes of death in developing countries. The present study was aimed with the 572 cases of road traffic accidents brought to the hospital for medico legal post mortem examination to study the distribution, nature and types of injuries received during fatal RTAs. Out of the 572 cases, 68.8% were males, while 31.1% were females. Maximum number (47.9%) of cases is found in the age group of 20-30 years and belong to employed or job holder group. In the present study, the maximum death cases were seen in pedestrians and maximum number of cases had injuries on Head with mostly sustained Abrasions. Present study also shows that majority death took place in the hospital followed by cases at accident site and cases during transportation. To conclude, A strict strategic plan and public awareness about the traffic rules, traffic sense, and more strict enforcement of roadside rules would be the best solution to the high RTA. Key Words: Accidents; RTA; Death; injuries.
INTRODUCTION Among all traffic accident in developed and developing countries worldwide, road traffic accidents claim largest toll of human life and tend to be the most serious problem leading cause of death for young people. According WHO (2016) it is estimated that a total of 1.2 million of deaths recorded globally1. RTAs have impacted negatively to society and its economy. It has claimed the largest toll of human life and tends to be the most serious problem all over the world2. Currently motor vehicle accidents rank 9th in order of disease burden and are projected to be ranked third in the year 20203. The causes of RTAs depends upon a number of factors, human errors, some are alcohol related, driver fatigue, poor traffic sense, mechanical fault of vehicle, speeding and overtaking, violation of traffic rules, poor road conditions, traffic congestion, or mental illness experiences higher crash and violation rates4. Road safety involves three major components: the road system, the human factor and the vehicle element. These three elements are inter-linked through geo-referenced traffic events and provide the basis for road safety analyses and attempts to reduce the number of road traffic incidents and improve road safety5. There is some evidence that the numbers of RTAs are plateauing, with RTAs spiking in the developing world, the trend line in high-income countries was moving in the opposite direction. Between 1990 and 2015, average RTI mortality in all OECD countries declined from 22 to 8 per 100,000. In developing countries, the proportion of serious injured and killed casualties are higher than in the developed countries. An analysis of cross-sectional data on road traffic related deaths has shown that the poorest countries have highest road traffic related mortality rates6. In developing countries there are some peculiarities regarding the accident profiles. A study done in Calcutta India, reported that there are some host (human) factors (such as the behaviour of drivers, pedestrians and cyclist behaviours) and seasonal factors (weather and time) that contribute to fatal road traffic accidents7. Overall, most traffic accidents occurred on main roads (highways) and in the majority of cases pedestrians were found to be at fault during crossing the roads8. Studies done worldwide have shown that road traffic accidents are the leading causes of death of many adolescents and young adults9. There is evidence that using minimum safety standards, crash worthiness improvement in vehicles, seatbelts use laws and reduced alcohol use can substantially reduce deaths on the road10. The curiosity of this study under its objective seeks to fill the gap of knowledge which exists by identifying the distribution, nature and types of injuries received during fatal RTAs, and to suggest useful road safety measures.
MATERIALS AND METHODS This was a prospective study was conducted at the Department of Forensic Medicine and Toxicology Osmania Medical College, Hyderabad during the period of March 2015 to March 2016. All the 572 cases of road traffic accidents brought to the hospital for medico legal post mortem examination were the subjects of the study. Those who participated in the study were assured of confidentiality of the information given. They were too requested to give voluntary informed consent prior to collecting data from them. Necessary information for the study was gathered from Police, inquest report and the date, time and place of accident, were collected from the relatives, friends, and neighbors of the victims was also taken separately.
RESULTS
Table 1: Socio-demographic profile of the subjects
In the present study, out of the 572 cases, 68.8% were males, while 31.1% were females. Age wise distribution of the cases is divided in to four groups. It is observed that maximum number (47.9%) of cases are found in the age group of 20-30 years, while 31.6%, were in the age group 31-40 years. In addition, 13.6% were between 41-50 years of age, while 6.8% were 51 years and above (Table 1). In this study maximum cases were belonging to employed or job holder group which constitute 41.2%, while 23.8% were students. Business or farmers formed 12.7% and others include 8.9%. Majority of those who travelled frequently included students and formally employed people (Table 1).
Table 2: Distribution of cases according to Road users
In the present study, the persons died due to RTA were as follows. Out of 572 cases 10.3% were pedestrian, 12.7% were pedal cyclist, 24.1% were motor cyclist, 28.4% were Light Vehicle users and 16.9% were Heavy Vehicle users, where as 7.3% cases reasons were unknown. There was a significant relationship between the type of vehicle perceived to be involved in RTAs and the actual vehicle which caused RTAs (Table 2).
Table 3: Sites of injuries in road traffic accidents
In the present study, the injuries were distributed according to the presence on various body regions in relation to type of victim. Many persons have injuries over single, double or more body regions. Maximum number of cases had injuries on Head 169 (29.5%) out of 572 cases. Further 86 cases had injury over thorax region. Injuries to abdominal region was seen in 81 cases and pelvic includes 62 cases and multiple sites include 53cases (Table 3).
Table 4: Distribution of cases according to type of external injuries
In the present study, mostly sustained Abrasions was seen in 320 cases followed by contusions in 96 cases and laceration seen in 16 cases, Blunt and Incised wounds were seen in 28 and 29 cases only respectively (Table 4).
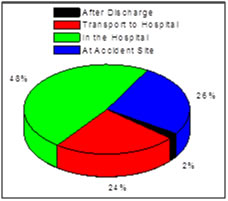
Figure 1: Place of death among fatal road traffic injuries From the chart above, majority (48%) death took place in the hospital followed by 26% of cases died at accident site and 24% of cases died during transportation and 2% of cases died after discharge from hospital (Figure 1).
DISCUSSION Accidents are a preventable cause of death. Unfortunately, it accounts for a large number of deaths in many societies. Accident is the result of a combination of factors such as human error, road defects, engineering defects of the vehicle, non-availability of pedestrian facility, cyclist facility, circumstantial factors such as weather condition, visibility but fault of driver results in 80% of accidents includes over speeding, overtaking, intake of alcohol and other drugs and others-act of talking over cell phones, driver fatigue, distractions and etc.11,12 In the present study, a total of 572 cases of fatal road traffic accidents have been studied in respect to distribution, nature and type of injuries. The present study, 68.8% were males, while 31.1% were females. Males outnumbered females in all categories of accidental deaths. The differences may be due to the lack of attention and negligence of safety protocols among males. Age wise distribution showed that maximum numbers of cases are found in the age group of 20-30 years, belonging to employed or job holder group which constituted 41.2% of the total study population. Singh & Dhattarwal have reported that maximal fatal accidents have occurred in the age group of 21- 30 years and a preponderance of males is seen13 In the present study, the persons died due to RTA were maximum from Light Vehicle users group when compared with pedestrian, pedal cyclist, motor cyclist and Heavy Vehicle users. This can be attributed to their high speed, greater momentum, presence of single space roads, overtaking, volume of traffic etc. Our findings are in general agreement with other studies14. Present study also showed the distribution of injuries in RTA individuals, many of the cases have injuries over single, double or more body regions. Maximum number of cases had injuries on head when compared with other parts of the body. In majority of cases, brain has been chiefly injured followed by Upper and lower extremities, Thorax and abdomen and pelvis respectively. A higher incidence of brain injury has also been reported by other workers15,16. The injuries which were common in road accidents victims are abrasions, contusions, lacerations, incised wounds, fractures and injuries involving internal organ. In the present study, most of the cases have shown abrasions in 360 cases followed by Contusions in 96 cases and laceration seen in 16 cases, Blunt and Incised wounds were seen in 28 and 29 cases only respectively. Our study was in contrast to earlier studies17. Regarding period of survival of fatal RTA victims, we have noted that a great majority of victims have died in the hospital followed by at accident site and during transportation after discharge from hospital. Our findings are in general agreement with those of18. It may be concluded that there is an urgent need to educate which is the most important factor in reducing those kinds of deaths and are therefore preventable. A strict strategic plan and public awareness about the traffic rules, traffic sense, and more strict enforcement of roadside rules would be the best solution to the high RTA.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.